This book was created to help patients and families better understand neurological conditions in clear and simple language. Artificial intelligence tools were used to organize information and improve readability, always under the guidance and review of the author. All medical explanations, examples, and recommendations have been carefully verified to ensure accuracy and relevance for patient education.
Introduction
Neurology, the study of the brain and nervous system, can often seem overwhelming for patients and families. Medical terms may sound complex, and understanding what is happening in the body can be confusing. This book was created to make neurological conditions easier to understand, using clear and simple explanations that bridge medical knowledge with patient education.
This book is designed as a companion to the A to Z Neurology for Physicians textbook. It follows the same structure but focuses entirely on individual neurological diseases, explained in everyday language. Physicians can use this book as an educational tool to help patients and their families understand specific conditions discussed during clinical visits. It also serves as a helpful guide for anyone who wants to learn more about neurological disorders in a concise and approachable way.
While this book simplifies many medical ideas for easier understanding, it does not replace professional medical advice or serve as a comprehensive reference. Readers are encouraged to consult qualified healthcare professionals and verified medical resources for further information and personalized guidance.
By improving understanding of neurological conditions, this book aims to empower patients and caregivers to take a more active role in their healthcare journey and foster better communication between doctors and patients.
Vijay Renga, MD
Acute Disseminated Encephalomyelitis (ADEM)
What is it?
ADEM is a short-term inflammation of the brain and spinal cord that usually appears after an infection.
It happens when the body’s defense system mistakenly attacks the brain’s protective coating.
The condition causes temporary problems with thinking, balance, and muscle control.
ADEM most often affects children and young adults.
It usually occurs only once, and most people make a full recovery.
What causes it?
ADEM often develops one to three weeks after a viral or bacterial infection.
The immune system becomes confused and attacks healthy nerve tissue.
Rarely, it may follow a vaccination, though this is uncommon.
The exact cause isn’t fully understood, but it involves an overactive immune response.
It’s not contagious—you can’t spread it to others.
How is it diagnosed?
Doctors consider recent illness, symptoms, and examination findings.
An MRI scan shows small spots of inflammation in different parts of the brain and spinal cord.
A spinal tap can check for signs of infection or inflammation.
Blood tests help rule out other causes such as multiple sclerosis.
The combination of test results and symptoms confirms the diagnosis.
What is the treatment?
High-dose steroids are given by vein to reduce swelling and calm the immune system.
If steroids don’t work, treatments like plasma exchange or IV immunoglobulin can be used.
Supportive care includes rest, fluids, and physical or occupational therapy.
Seizures, headaches, or fever are treated as needed.
Most people start to feel better within days of treatment.
What is the prognosis?
Most patients recover fully within weeks to months.
A few may have mild lasting weakness or coordination issues.
Recurrence is rare.
Regular follow-up helps ensure the brain heals completely.
AIDP is a nerve disorder that causes sudden weakness starting in the legs and moving upward.
It’s the most common form of Guillain–Barré syndrome.
The immune system mistakenly attacks the nerves’ protective covering.
This slows down or blocks the messages between the brain and the muscles.
With proper treatment, most people recover well.
What causes it?
It often begins one to three weeks after an infection such as a cold or diarrhea.
The immune system becomes overactive and attacks nerve tissue instead of germs.
Certain bacteria and viruses are more likely to trigger it.
It’s not inherited or contagious.
The exact reason why it happens to some people is not fully known.
How is it diagnosed?
Doctors look for symmetrical weakness that begins in the legs and loss of reflexes.
A spinal tap shows high protein levels but very few cells in the fluid.
Nerve tests show slower electrical signals due to nerve damage.
MRI scans may show swelling of the nerve roots in the spine.
Other similar conditions are ruled out through testing.
What is the treatment?
Hospital care is needed to watch breathing, heart rhythm, and blood pressure.
IV immunoglobulin (IVIG) or plasma exchange helps calm the immune system.
Steroids are not useful and are not recommended.
Physical therapy helps prevent stiffness and improves muscle recovery.
Supportive care, including nutrition and emotional support, aids recovery.
What is the prognosis?
Most people recover strength within a few months.
Some may have mild lingering weakness or fatigue.
Early treatment leads to a faster and more complete recovery.
Severe cases may take longer but usually improve with rehabilitation.
The condition rarely returns once it has resolved.
Alcohol and Neurology
What is it?
Long-term heavy drinking can harm the brain and nerves, leading to balance, memory, and movement problems.
Alcohol affects how nerve cells talk to each other and can shrink certain brain areas.
Common effects include poor coordination, confusion, numbness in the feet or hands, and trouble walking.
Some people develop specific conditions such as Wernicke-Korsakoff syndrome or cerebellar degeneration.
The brain changes are often partly reversible if alcohol use stops early.
What causes it?
Alcohol itself is toxic to nerve and brain cells when used over many years.
Drinking heavily often leads to poor diet and vitamin B1 (thiamine) deficiency, which damages the brain.
Low thiamine levels cause Wernicke’s encephalopathy and memory loss (Korsakoff’s syndrome).
The cerebellum, which controls balance, is especially sensitive to alcohol damage.
Other toxins and liver problems from alcohol can worsen brain function.
How is it diagnosed?
Doctors look for symptoms such as unsteady walking, slurred speech, or numbness in the limbs.
They ask about drinking habits and check for signs of poor nutrition.
Blood tests can show low vitamin levels and liver changes from long-term drinking.
MRI scans may show shrinkage in the cerebellum or other parts of the brain.
Nerve tests can reveal damage to the peripheral nerves in the hands and feet.
What is the treatment?
The most important step is stopping alcohol use completely.
High-dose vitamin B1 (thiamine) is given right away, especially before receiving any sugar or glucose.
Eating a balanced diet with vitamins helps the brain and nerves heal.
Physical and occupational therapy can improve coordination and movement.
Counseling and support groups help maintain sobriety and emotional recovery.
What is the prognosis?
If alcohol use stops early, many symptoms can improve or even disappear.
Memory loss and nerve damage may be partly reversible, though some effects can last.
Continued drinking leads to worsening brain and nerve injury.
Early vitamin replacement can prevent Wernicke-Korsakoff syndrome from becoming permanent.
Long-term recovery depends on full abstinence, good nutrition, and consistent follow-up.
Alzheimer’s Disease
What is it?
Alzheimer’s disease is a brain condition that slowly causes problems with memory and thinking.
It is the most common cause of dementia in older adults.
Over time, people may forget names, places, and daily routines.
The disease affects how brain cells communicate and eventually leads to their loss.
It develops gradually, starting with forgetfulness and progressing to more severe confusion.
What causes it?
The disease happens when harmful proteins build up in the brain and damage nerve cells.
These proteins—called amyloid and tau—disrupt brain cell connections.
Age, family history, and certain genes increase the risk.
Poor heart health, diabetes, and head injuries can also raise the risk.
The exact cause isn’t fully known, but lifestyle and genetics both play roles.
How is it diagnosed?
Doctors start by asking about memory, mood, and daily function.
Simple tests check thinking, attention, and problem-solving abilities.
MRI or CT scans can show shrinkage in memory-related brain areas.
Blood and spinal fluid tests help rule out other causes of memory loss.
Early diagnosis allows better planning and support for the patient and family.
What is the treatment?
Medicines like donepezil or memantine can help with memory and behavior.
Staying mentally and socially active slows down memory decline.
A healthy diet, regular exercise, and good sleep support brain health.
Counseling and support groups help families manage daily challenges.
New treatments are being developed to target the brain changes directly.
What is the prognosis?
Alzheimer’s disease usually worsens slowly over several years.
Early stages involve forgetfulness, while later stages affect all daily activities.
With care and treatment, many people can live meaningful lives for years.
The focus of treatment is comfort, safety, and quality of life.
Support from caregivers and medical teams makes a major difference in long-term well-being.
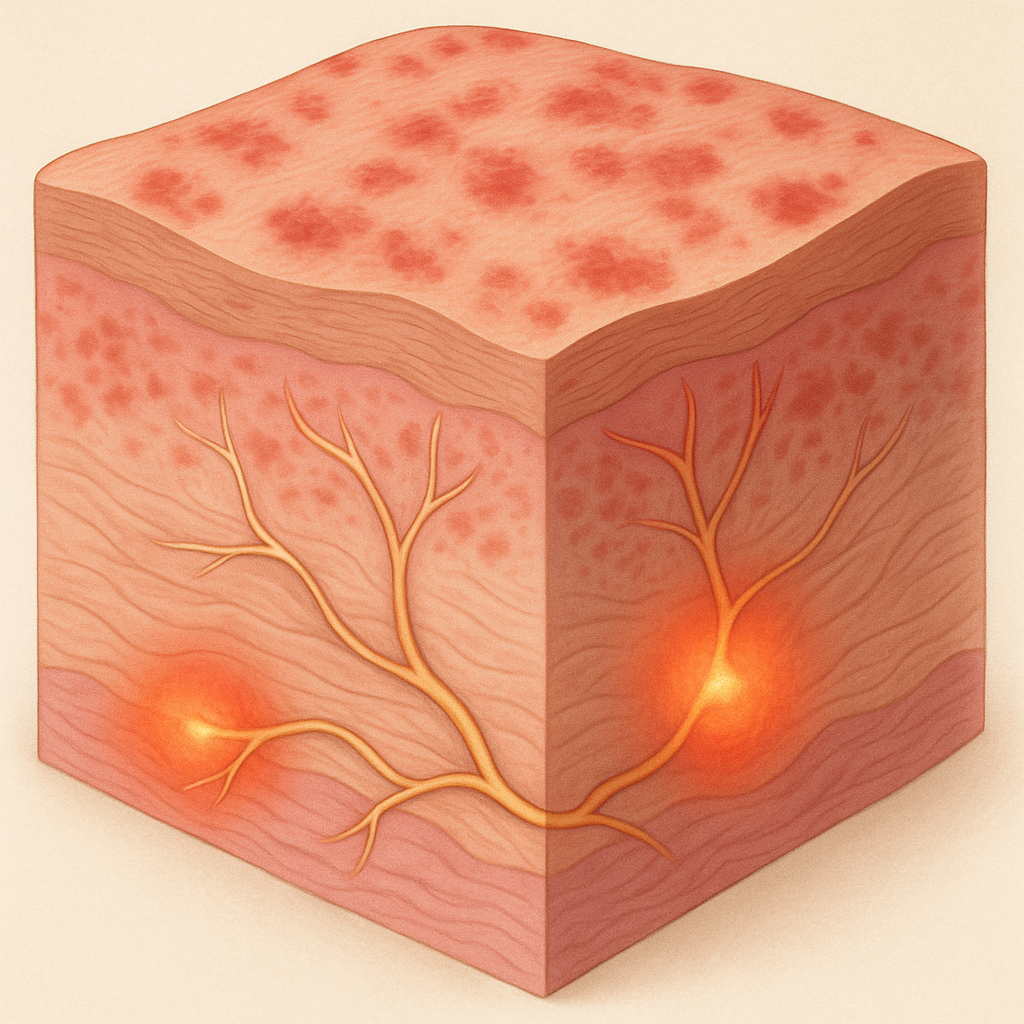
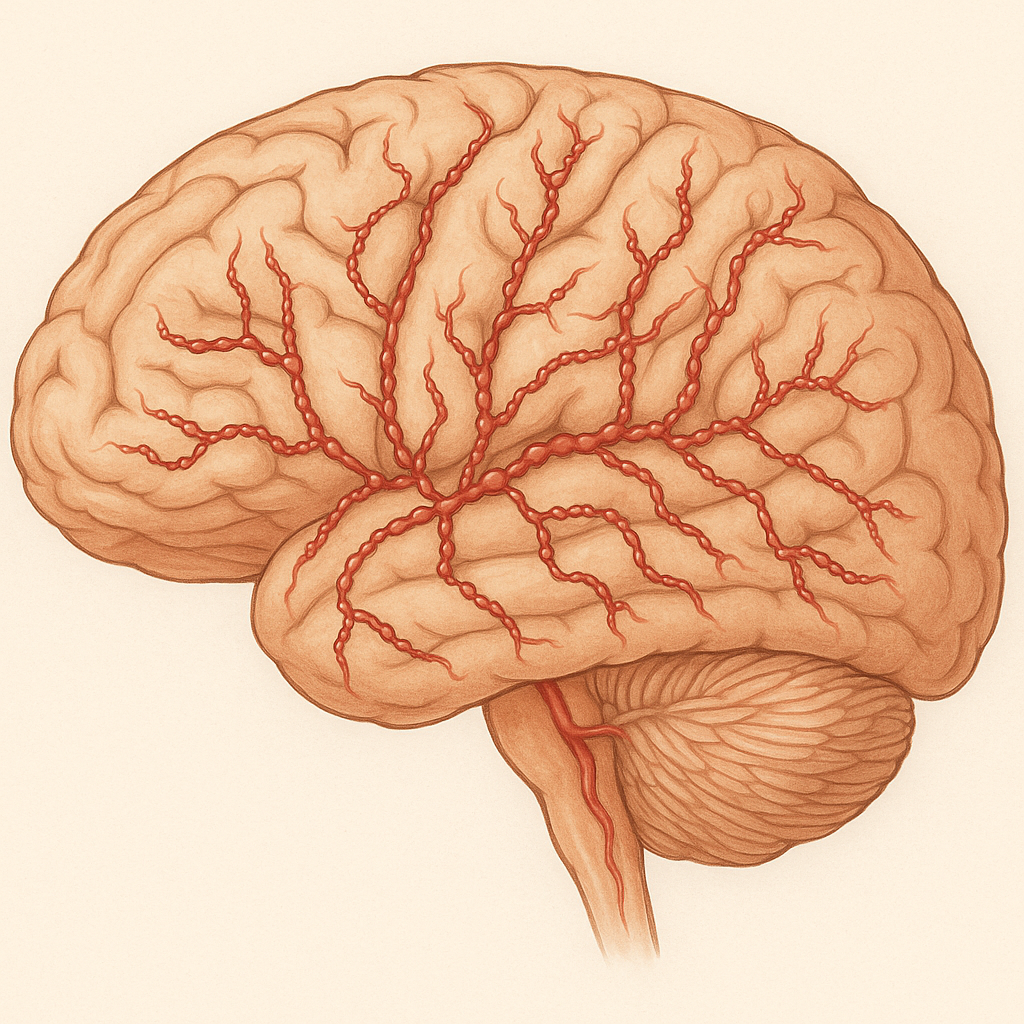
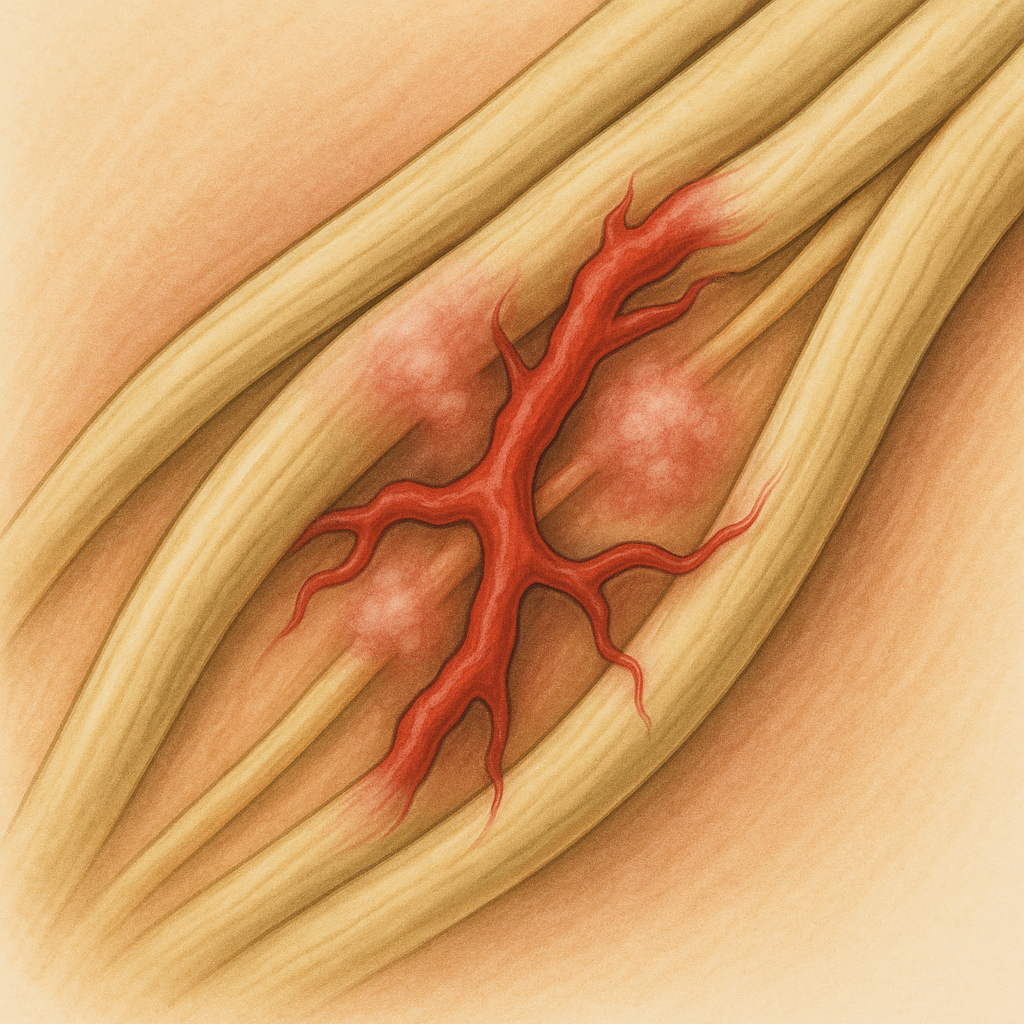
Amyloid Angiopathy
What is it?
Amyloid angiopathy (CAA) is a condition in which abnormal protein called amyloid-\(\beta\) builds up in the walls of small blood vessels in the brain.
This weakens the vessels, making them more likely to bleed and causing lobar intracerebral hemorrhages.
It mainly affects older adults and is a common cause of spontaneous (non-hypertensive) brain bleeding.
The same protein is also involved in Alzheimer’s disease, linking the two conditions.
CAA can also cause small “silent” bleeds, cognitive changes, or transient neurological symptoms.
What causes it?
The disease is caused by gradual deposition of amyloid-\(\beta\) (especially A\(\beta\)40) in the walls of cortical and leptomeningeal arteries.
These deposits damage and weaken the vessel wall, leading to bleeding.
The underlying process relates to problems with amyloid clearance from the brain.
Genetic factors such as APOE \(\varepsilon\)2 and \(\varepsilon\)4 increase risk.
It is not caused by high blood pressure, trauma, or infection.
How is it diagnosed?
MRI scans show typical findings — multiple small “microbleeds” in the cortex and cortical superficial siderosis (thin lines of old blood on the surface).
CT scans help detect acute bleeds, usually in the lobar (outer) brain regions.
The diagnosis is made using the Boston Criteria, based on clinical and MRI findings.
A brain biopsy is rarely needed, only if other causes like vasculitis are suspected.
Other conditions such as hypertensive bleeds or vascular malformations must be ruled out.
What are the symptoms?
Sudden weakness, speech disturbance, or confusion due to lobar hemorrhage.
Recurrent episodes of lobar bleeding over time.
Progressive memory loss and cognitive decline in some patients.
Less commonly, seizures or headaches during acute bleeds.
What is the treatment?
There is no cure, but treatment aims to prevent further bleeding and manage symptoms.
Strict blood pressure control is essential to reduce recurrence risk.
Avoid blood thinners and antiplatelet medications if possible.
Seizures are treated with appropriate antiepileptic drugs.
Physical and cognitive rehabilitation can help recovery after bleeds.
Experimental therapies targeting amyloid clearance are under study.
What is the prognosis?
The outlook depends on the severity and recurrence of bleeding.
Many patients recover from a single bleed, but recurrent episodes can lead to lasting disability or dementia.
Avoiding risk factors and close medical follow-up help reduce complications.
Long-term management focuses on maintaining independence and preventing further hemorrhage.
Supportive care and monitoring for cognitive symptoms improve quality of life.
Amyloid Neuropathy
What is it?
Amyloid neuropathy is a nerve problem caused by abnormal protein deposits called amyloid.
These proteins build up in and around nerves, affecting their ability to send signals.
It often causes tingling, burning, or numbness in the feet and hands.
Some people also have dizziness, stomach problems, or trouble controlling blood pressure.
The condition can be inherited or develop later in life as part of another illness.
What causes it?
It occurs when certain proteins fold the wrong way and form sticky deposits that damage nerves.
These proteins can come from genetic changes (inherited) or from disorders of blood cells.
In some people, long-term inflammatory diseases can also lead to amyloid buildup.
The deposits block blood supply and nutrition to nerve fibers.
Over time, this causes nerve fibers to die and symptoms to progress.
How is it diagnosed?
Doctors suspect the diagnosis when there is numbness, pain, and dizziness that worsen slowly.
A nerve test can show how well the nerves are working and reveal damage.
A small biopsy of fat or nerve tissue confirms amyloid by special staining under the microscope.
Blood and genetic tests help find the type of amyloid and guide treatment.
Scans or heart and kidney tests may check if other organs are also affected.
What is the treatment?
Treatment focuses on stopping more amyloid from forming and relieving symptoms.
Inherited forms may be treated with new medicines that block or silence the abnormal protein.
For acquired cases, chemotherapy or stem cell therapy may remove the source of amyloid.
Pain medicines, blood pressure support, and diet changes help manage daily symptoms.
Early treatment and healthy lifestyle changes can slow or even improve nerve damage.
What is the prognosis?
With early diagnosis and proper treatment, many people can control the disease.
Some nerve damage may improve once amyloid production is stopped.
Delayed treatment can lead to permanent weakness and loss of sensation.
The outcome depends on the type of amyloid and how much other organs are involved.
Regular follow-up helps track progress and adjust therapy as needed.
Amyotrophic Lateral Sclerosis (ALS)
What is it?
ALS is a disease that affects the nerve cells that control muscles.
These nerves gradually stop working, causing weakness and muscle wasting.
It can start in the hands, feet, or speech muscles and slowly spread to other areas.
The condition does not affect thinking or senses in most people.
Over time, the muscles that help with breathing and swallowing also weaken.
What causes it?
Most cases occur without a clear cause, but about one in ten is inherited.
Changes in certain genes can make nerve cells more sensitive to damage.
Chemicals that overstimulate or stress nerve cells may play a role.
Inflammation and poor energy supply to the nerves also contribute.
The condition is not caused by infections or lifestyle choices.
How is it diagnosed?
Doctors diagnose ALS based on the pattern of weakness and muscle changes.
Nerve and muscle tests (EMG and NCS) show how well the nerves send signals.
MRI scans help rule out other conditions like spinal cord problems.
Blood and genetic tests may be used to confirm or exclude inherited forms.
A neurologist experienced in motor neuron diseases usually confirms the diagnosis.
What is the treatment?
There is no cure, but medicines like riluzole and edaravone can slow disease progression.
Breathing and swallowing support are key parts of care as symptoms advance.
Physical, speech, and occupational therapy help maintain mobility and communication.
Nutrition and emotional support improve comfort and quality of life.
New research is exploring treatments that target the disease at a genetic level.
What is the prognosis?
ALS progresses at different rates in different people.
Many people live for several years after diagnosis, and some live much longer.
Early multidisciplinary care improves both comfort and survival.
Breathing support can greatly extend life expectancy.
Ongoing research gives hope for better treatments and possible future cures.
Anoxic Brain Injury
What is it?
Anoxic brain injury happens when the brain does not get enough oxygen for several minutes.
It often occurs after a cardiac arrest, drowning, or choking.
Without oxygen, brain cells begin to die quickly, especially in areas that control memory and movement.
Some people recover partially, while others may remain in a coma or have lasting disabilities.
The severity depends on how long the brain went without oxygen and how quickly help arrived.
What causes it?
The main cause is a complete stop or severe drop in oxygen supply to the brain.
Common triggers include cardiac arrest, suffocation, severe asthma, or drug overdose.
Stroke, carbon monoxide poisoning, or electrical shock can also cause it.
When blood flow stops, brain cells lose energy and begin to break down.
Even after oxygen returns, inflammation and toxins can cause more damage.
How is it diagnosed?
Doctors suspect it when a person does not wake up after oxygen loss.
Brain scans such as MRI or CT show which areas are damaged.
EEG tests measure brain activity and can help predict recovery chances.
Blood tests may show signs of stress or injury to brain cells.
Doctors use all this information together to understand the extent of the injury.
What is the treatment?
The first step is restoring oxygen and blood flow as soon as possible.
Cooling the body (targeted temperature therapy) can help reduce further brain damage.
Doctors control seizures, maintain normal blood pressure, and prevent infections.
Once stable, rehabilitation helps with movement, speech, and memory recovery.
Family support and therapy are key for long-term improvement and quality of life.
What is the prognosis?
Recovery depends on how long the brain went without oxygen and the amount of damage.
Some people may wake up and recover slowly over weeks or months.
Others may have lasting problems with memory, speech, or movement.
Severe cases may lead to coma, vegetative state, or death.
Early resuscitation and care greatly improve the chances of recovery.
Anterior Interosseous Nerve Syndrome (AINS)
What is it?
AINS is a nerve problem that causes weakness in certain hand and forearm muscles.
It affects a small branch of the median nerve that controls thumb and index finger movement.
People with AINS may have trouble making the “OK” sign with their fingers.
It usually causes weakness but no numbness or tingling.
The condition often improves on its own but may take several months.
What causes it?
It can happen when the nerve is squeezed by tight muscles or tendons in the forearm.
Sometimes it follows a viral infection or inflammation of the nerve (neuritis).
Overuse or repetitive arm movement may contribute in some cases.
Rarely, trauma or surgery near the elbow can damage the nerve.
In many people, the exact cause is never found.
How is it diagnosed?
Doctors look for weakness in the thumb and index finger without loss of feeling.
The “pinch test” helps show the classic triangular “OK” sign weakness.
Nerve and muscle tests (EMG) confirm which muscles are affected.
MRI or ultrasound may be done to check for nerve compression or swelling.
The diagnosis is mostly clinical, based on symptoms and physical exam.
What is the treatment?
Most cases improve naturally over time without surgery.
Rest, gentle stretching, and physical therapy help recovery.
Pain and inflammation can be managed with medications if needed.
If the nerve does not recover after 6–12 months, surgery may relieve pressure.
Recovery is usually good, and most people regain near-normal hand strength.
What is the prognosis?
Many patients recover fully within 3 to 6 months.
Some may have mild, lasting weakness in fine finger movements.
Early physical therapy helps prevent stiffness and speed up healing.
Inflammation-related cases respond faster than those caused by compression.
Overall, the long-term outlook is excellent for most people.
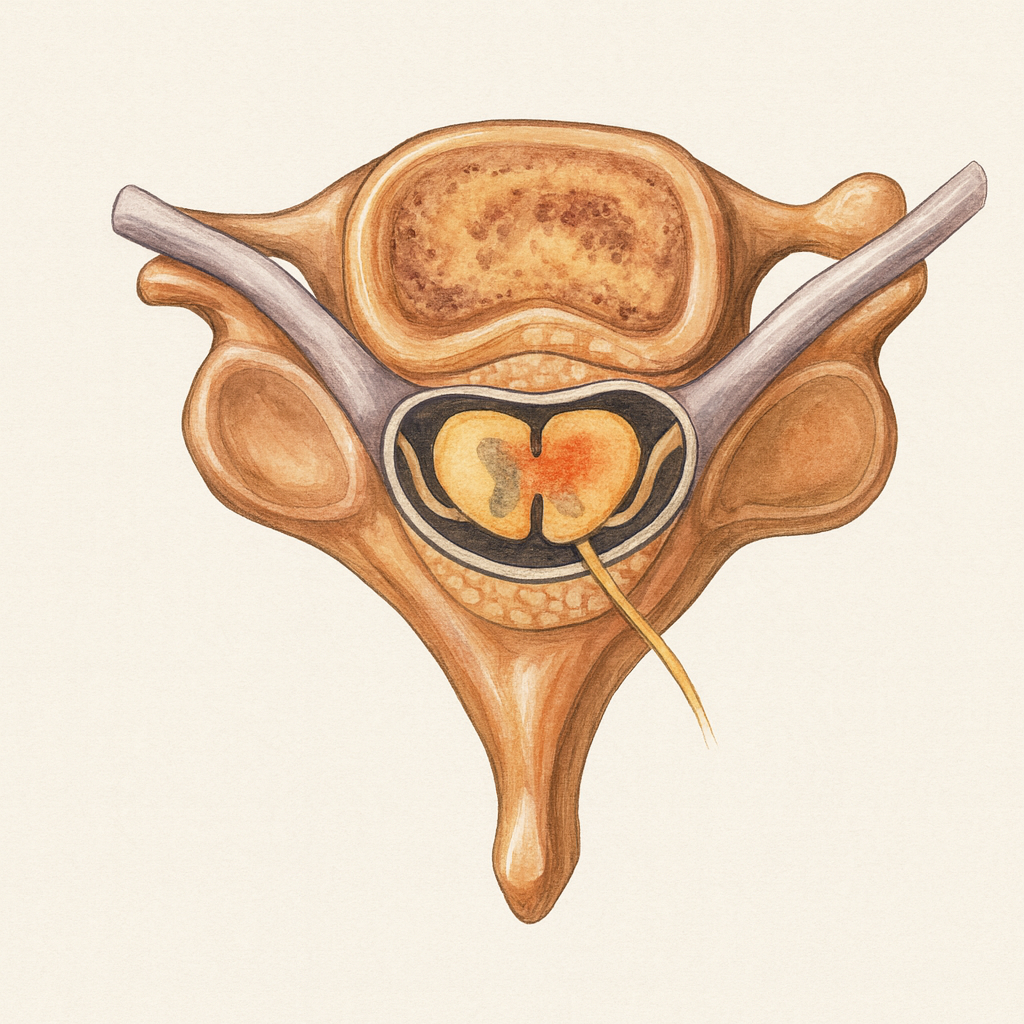
Arachnoiditis
What is it?
Arachnoiditis is a long-term inflammation of one of the coverings around the spinal cord called the arachnoid membrane.
It causes thickening and scarring that can trap and irritate the spinal nerves.
People with this condition often have severe, burning pain in the lower back and legs.
It can also affect bladder and bowel control in some people.
Arachnoiditis is chronic, meaning symptoms may last for years and need ongoing care.
What causes it?
The most common cause is irritation from spinal surgery, injections, or infections.
Past spinal procedures, especially epidural or intrathecal injections, can lead to inflammation.
Rare causes include trauma, bleeding around the spinal cord, or chemical irritation.
Sometimes infections like tuberculosis or syphilis can trigger it.
In many cases, a combination of surgical and inflammatory factors is involved.
How is it diagnosed?
Doctors suspect it when back and leg pain persist after surgery or spinal injections.
MRI scans show scarring, thickened tissues, and clumping of nerve roots.
Nerve tests may show changes in multiple nerve roots, though they are not specific.
A detailed history of past spine procedures helps confirm the diagnosis.
Other conditions like spinal stenosis or nerve injury must be ruled out.
What is the treatment?
There is no cure, but treatments can ease pain and improve function.
Medications like gabapentin, pregabalin, or duloxetine help reduce nerve pain.
Physical therapy and gentle stretching improve mobility and strength.
In some cases, spinal cord stimulators or pain management programs are helpful.
Surgery is rarely done, as it may worsen scarring, but may help selected patients.
What is the prognosis?
The condition is long-term but varies from person to person.
Many patients live with chronic pain that can be managed with treatment.
Early diagnosis and a team approach improve comfort and function.
Emotional support and counseling can help with coping and quality of life.
Regular follow-up helps adjust therapy as symptoms change over time.
Arnold–Chiari Malformation
What is it?
Arnold–Chiari malformation is a condition where part of the brain (the cerebellum) sits too low and pushes into the spinal canal.
It can block the normal flow of spinal fluid, leading to pressure and neurological symptoms.
Some people are born with it and may not notice symptoms until adulthood.
It is often found by accident on a brain scan done for other reasons.
There are several types, with Type I being the mildest and most common in adults.
What causes it?
It usually develops before birth due to the back of the skull being too small.
The tight space pushes brain tissue downward through the opening at the base of the skull.
In some people, it can appear later due to spinal fluid pressure changes or surgery.
Genetic and environmental factors both play a role in its development.
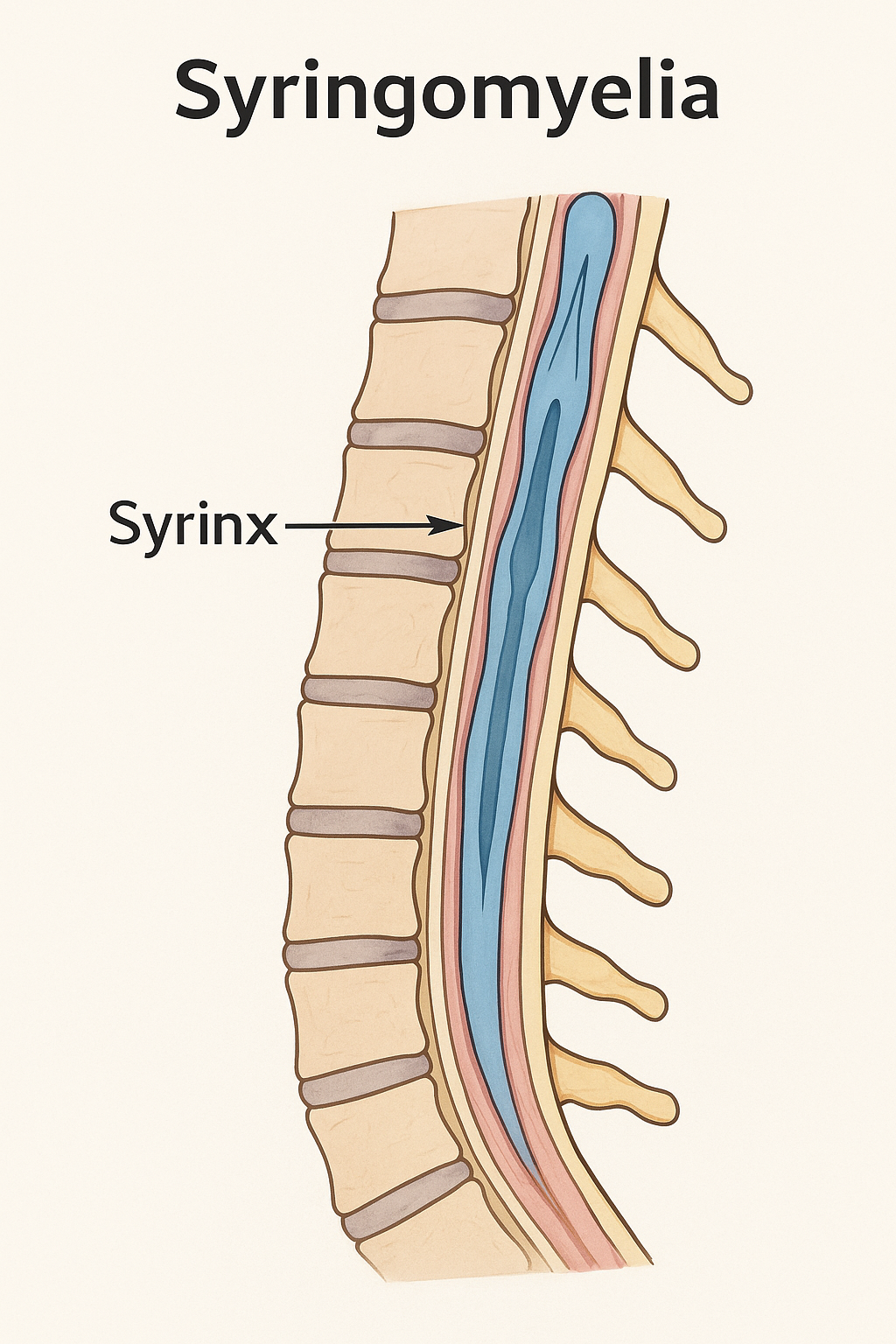
Sometimes it is found along with other spinal conditions like syringomyelia.
How is it diagnosed?
MRI scans of the brain and neck show how far the brain tissue has moved down.
A special MRI (cine MRI) can check if spinal fluid is blocked at the skull base.
Doctors may do nerve and balance tests to look for brainstem involvement.
The diagnosis is usually clear from imaging combined with symptoms.
In children, prenatal ultrasound or MRI can sometimes detect it before birth.
What is the treatment?
Mild cases with no symptoms may only need regular monitoring.
Surgery is recommended if headaches, balance issues, or numbness become severe.
The most common surgery removes a small part of bone to make more space for the brain.
If spinal fluid buildup (hydrocephalus) occurs, a shunt may be placed to drain it.
Physical therapy helps improve coordination and reduce neck stiffness after recovery.
What is the prognosis?
Most people with mild forms live normal, active lives.
Surgery often relieves pressure and improves headaches or balance problems.
Symptoms may return if scarring or fluid blockage recurs, requiring follow-up.
Early diagnosis and treatment improve long-term outcomes.
Lifelong monitoring ensures any new problems are caught early.
Arsenic Toxicity
What is it?
Arsenic toxicity occurs when the body is exposed to excessive amounts of arsenic, a naturally occurring element found in groundwater, industrial emissions, and contaminated food sources.
Chronic exposure most commonly affects the skin, peripheral nerves, and internal organs.
It can lead to neurological, dermatological, and systemic manifestations.
Arsenic exists in both organic and inorganic forms, with the inorganic type being more toxic.
Long-term exposure is a major global health concern, especially in areas with contaminated well water.
What causes it?
Chronic exposure to arsenic-contaminated groundwater is the most common cause worldwide.
Occupational exposure occurs in industries such as mining, smelting, and pesticide manufacturing.
Arsenic binds to sulfhydryl groups and disrupts cellular respiration, impairing mitochondrial energy metabolism.
It generates reactive oxygen species, leading to oxidative stress, DNA damage, and apoptosis.
Genetic and nutritional factors can modify susceptibility to arsenic toxicity.
How is it diagnosed?
Diagnosis is based on clinical presentation, exposure history, and laboratory testing.
Urine arsenic measurement is the most reliable indicator of recent exposure.
Hair and nail arsenic levels reflect long-term exposure.
Nerve conduction studies show length-dependent axonal neuropathy, especially involving sensory fibers.
Water and environmental testing help identify the source of contamination.
What are the symptoms?
Tingling, numbness, and burning pain in the hands and feet due to peripheral neuropathy.
Skin hyperpigmentation, hyperkeratosis, and “raindrop” dark spots.
Transverse white lines on nails (Mees’ lines).
Non-healing skin ulcers and swelling of extremities.
Systemic features: fatigue, gastrointestinal distress, hepatotoxicity, nephrotoxicity, and anemia.
What is the treatment?
Remove the source of exposure and ensure access to safe drinking water.
Supportive treatment includes hydration, electrolyte correction, and management of acute symptoms.
Chelation therapy may be indicated for moderate to severe toxicity:
Dimercaprol (British Anti-Lewisite)
DMSA (succimer)
DMPS
Neuropathic pain is managed with medications such as gabapentin, duloxetine, or tricyclic antidepressants.
Rehabilitation and long-term monitoring help manage neurological sequelae and cancer risk.
What is the prognosis?
Prognosis depends on duration and severity of exposure.
Early diagnosis and removal from the exposure source greatly improve outcomes.
Peripheral neuropathy may partially recover, though some sensory loss can persist.
Long-term exposure increases the risk of skin, lung, and bladder cancers.
Public health measures and clean water initiatives are critical to prevent recurrence.
Autoimmune Autonomic Gangliopathy
What is it?
Autoimmune Autonomic Gangliopathy (AAG) is a rare condition where the body’s immune system attacks the nerves that control automatic body functions.
These nerves manage things like blood pressure, sweating, digestion, and bladder function.
When they are damaged, people can feel dizzy on standing, have constipation, or trouble urinating.
Unlike other nerve diseases, muscle strength and sensation are usually normal.
It can develop suddenly or gradually and may improve with immune treatments.
What causes it?
The immune system mistakenly attacks nerve receptors that help send signals between automatic nerves.
This blocks communication in the “autonomic ganglia,” where nerve signals are relayed.
Some cases are linked to infections, cancers, or other autoimmune diseases.
A blood test often shows antibodies against the ganglionic acetylcholine receptor (gAChR).
In many people, the exact trigger is not known.
How is it diagnosed?
Doctors suspect it when a person has severe blood pressure drops, dry mouth, and other body-control problems.
Special blood tests can look for antibodies that confirm the autoimmune cause.
Autonomic tests, such as tilt-table or sweat tests, show how the nervous system reacts.
MRI or scans may be done to rule out cancer or other diseases.
Diagnosis combines symptoms, test results, and exclusion of other causes.
What is the treatment?
Treatment focuses on calming the immune system and easing symptoms.
Steroids, IV immunoglobulin (IVIG), or plasma exchange can reduce inflammation.
Medications like midodrine or fludrocortisone help control low blood pressure.
Other medicines manage constipation, urinary problems, and dry eyes or mouth.
Regular follow-up helps prevent relapses and detect new triggers early.
What is the prognosis?
Many people improve with prompt immune treatment, though recovery may take months.
Some experience long-lasting but manageable symptoms with ongoing care.
Relapses can happen, especially if treatment is delayed or incomplete.
The condition is rarely life-threatening when properly managed.
Early diagnosis offers the best chance for a strong recovery and stable long-term outcome.
Autoimmune Encephalitis
• What is it?
Autoimmune encephalitis is a condition where the body’s immune system mistakenly attacks the brain.
This attack leads to swelling and inflammation of brain tissue.
It can affect memory, thinking, behavior, and movement.
Symptoms often develop over days to weeks, making it feel sudden and alarming.
Although serious, it is treatable when identified early.
• What causes it?
The condition occurs when antibodies target proteins on brain cells.
These antibodies may develop after an infection, tumor, or for reasons that remain unknown.
Sometimes the immune system becomes overactive without a clear trigger.
Both adults and children can be affected.
Research continues to better understand why the immune system becomes misdirected.
• How is it diagnosed?
Diagnosis begins with a detailed history and neurological exam.
Doctors often perform blood tests and a lumbar puncture to look for specific antibodies.
MRI and EEG help detect inflammation or abnormal brain activity.
Sometimes the diagnosis is made even if antibody tests are negative.
Early recognition is important because treatment works best when started quickly.
• What is the treatment?
Treatment focuses on calming the immune system and reducing brain inflammation.
First-line therapies include steroids, IVIG, and plasma exchange.
If symptoms persist, stronger immunotherapies such as rituximab or cyclophosphamide may be used.
Patients often require supportive care, including seizure control and rehabilitation.
Many people improve significantly with timely treatment.
• What is the prognosis?
Most patients recover either fully or partially with appropriate therapy.
Improvement may take months, and rehabilitation can help restore memory and function.
A small number of patients may have lingering symptoms such as fatigue or mood changes.
Rarely, the disease can return and may require long-term monitoring.
Overall, prognosis is best when treatment begins early.
Axillary Neuropathy
What is it?
Axillary neuropathy is a problem with the nerve that helps lift your arm and feel the outer part of your shoulder.
This nerve, called the axillary nerve, controls the deltoid muscle that moves your shoulder.
When injured, it can cause weakness lifting your arm or numbness around the shoulder.
It often happens after shoulder injuries, such as a dislocation or fall.
Most people recover with rest and therapy, though severe cases may need surgery.
What causes it?
The axillary nerve can be stretched or pinched during a shoulder dislocation or fracture.
Surgery or injections near the shoulder can sometimes damage the nerve accidentally.
Repetitive overhead movements, such as in sports, can also irritate the nerve.
Less often, a tight space around the nerve or a lump can cause long-term pressure.
Rarely, inflammation or scarring can gradually affect nerve function.
How is it diagnosed?
Doctors look for weakness when lifting the arm and numbness over the outer shoulder.
They check the deltoid muscle, which is often smaller or weaker on the affected side.
Nerve tests (EMG or nerve conduction studies) can measure how well the nerve works.
Scans like MRI or ultrasound may show swelling, tears, or trapped nerves.
Other conditions like neck problems or rotator cuff tears are ruled out.
What is the treatment?
Most people start with rest and gentle physical therapy to keep the shoulder moving.
Pain medicine and avoiding further injury help the nerve heal.
If recovery is slow, doctors may suggest nerve stimulation or braces for support.
Surgery may be needed if the nerve is completely torn or trapped.
Regular checkups ensure the nerve is healing and muscle strength is returning.
What is the prognosis?
Many patients regain full or near-full shoulder strength within a few months.
Mild injuries usually recover without long-term effects.
Severe injuries can take longer and may leave some weakness or numbness.
Early diagnosis and therapy improve recovery chances.
With proper care, most people return to normal activities safely.
Bell’s Palsy
What is it?
Bell’s palsy is a sudden weakness or paralysis of one side of the face.
It happens when the facial nerve, which controls facial muscles, becomes inflamed.
The face may droop, and the person may not be able to close one eye or smile properly.
It can look alarming, but most cases are temporary.
The condition is not a stroke and usually improves over time with treatment.
What causes it?
It is often caused by swelling of the facial nerve due to viral infection.
The herpes simplex virus (the same one that causes cold sores) is thought to be a common trigger.
Cold weather, stress, or immune changes can sometimes play a role.
In some cases, no exact cause is found.
The nerve swelling temporarily blocks signals to the facial muscles.
How is it diagnosed?
Doctors recognize it from the sudden facial droop and inability to move facial muscles.
They check for other signs to make sure it’s not caused by a stroke or tumor.
Sometimes, MRI scans are done if symptoms are unusual or recovery is delayed.
No single test confirms it — diagnosis is mostly based on symptoms and exam.
Tests for infections or nerve studies may be done in unclear cases.
What is the treatment?
Steroid medicines like prednisolone help reduce nerve swelling and speed recovery.
Antiviral medications may be added, especially in more severe cases.
Eye protection with drops or taping is vital if the eyelid won’t close.
Gentle facial exercises help restore muscle strength.
Most people start improving within weeks and recover fully within months.
What is the prognosis?
Most people recover completely within 3 to 6 months.
Some may have mild weakness or tightness that lasts longer.
Early treatment gives a better chance of full recovery.
Recurrence is uncommon but can happen.
Permanent nerve damage is rare.
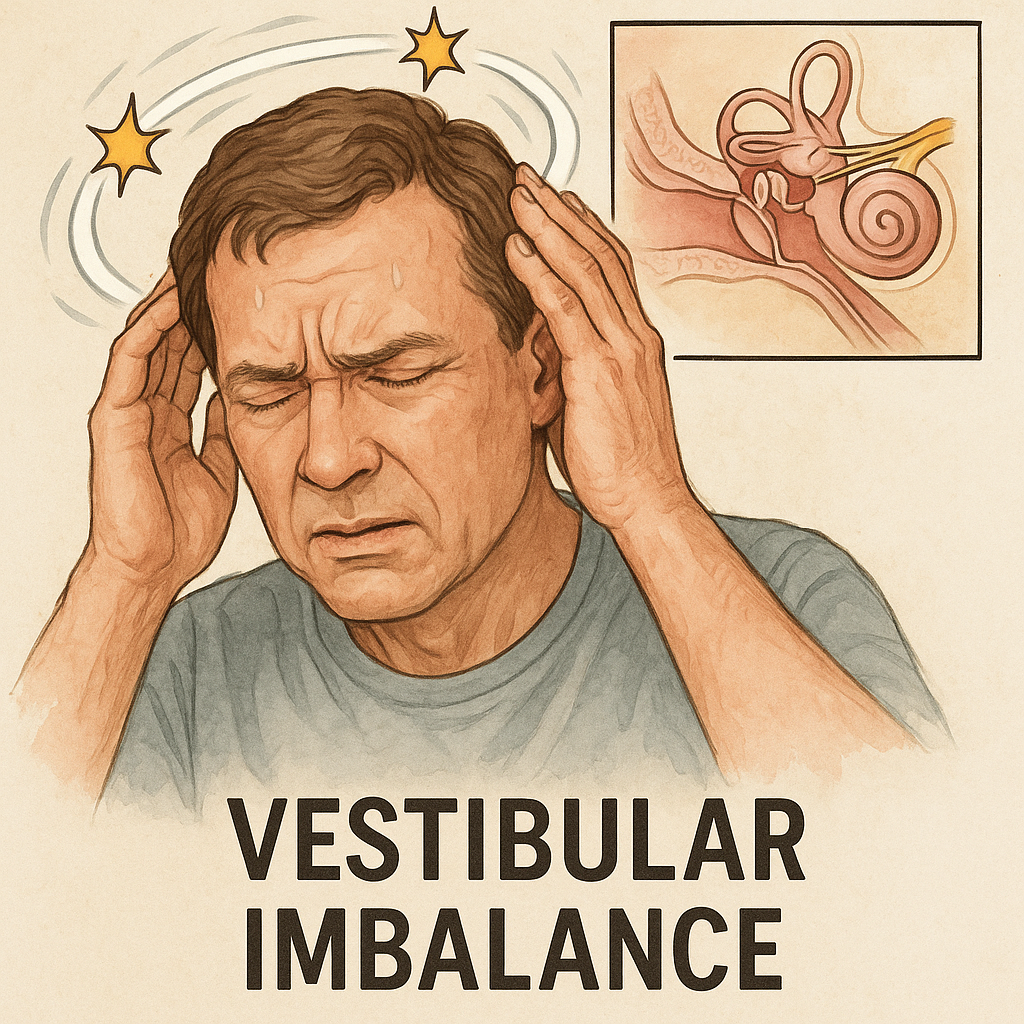
Benign Paroxysmal Positional Vertigo (BPPV)
What is it?
BPPV causes brief spinning sensations when you move your head, like turning in bed or looking up.
It happens when tiny crystals in the inner ear move out of place.
The spinning (vertigo) lasts seconds to a minute and then stops.
Hearing is not affected.
Though unpleasant, it is harmless and treatable.
What causes it?
The inner ear contains small crystals that help sense movement and balance.
When these crystals move into the wrong part of the ear canal, they disturb balance signals.
It can happen after a head injury, infection, or simply with age.
Sometimes it occurs without a clear reason.
Lying down or turning quickly can trigger episodes.
How is it diagnosed?
Doctors perform a simple head movement test called the Dix-Hallpike maneuver.
The test triggers the typical spinning sensation and specific eye movements.
Hearing and brain function tests are normal in BPPV.
Scans are rarely needed unless symptoms are unusual.
Diagnosis is based mainly on the pattern of dizziness.
What is the treatment?
Special head and body movements, like the Epley maneuver, reposition the crystals.
These are quick, noninvasive treatments done in the clinic.
Home exercises can help prevent recurrence.
Dizziness medicines are not usually needed.
Most people recover fully after one or two treatments.
What is the prognosis?
BPPV is very treatable and often resolves completely.
Some people may have mild recurrences over time.
Simple maneuvers can easily manage repeat episodes.
It does not cause permanent damage or hearing loss.
Avoiding prolonged bed rest can reduce the risk of recurrence.
Botulism
What is it?
Botulism is a rare but serious illness caused by a nerve toxin made by bacteria.
It leads to muscle weakness starting in the face and moving downward.
People stay awake and alert but become weak or paralyzed.
It can affect breathing and needs urgent hospital care.
With early treatment, most people recover fully.
What causes it?
The illness is caused by toxins from the bacteria Clostridium botulinum.
It can come from eating improperly canned or preserved food.
Babies can get it from swallowing spores that grow in their intestines.
It can also occur through wounds, especially in drug users.
The toxin blocks signals from nerves to muscles, causing paralysis.
How is it diagnosed?
Doctors look for typical signs — drooping eyelids, slurred speech, and descending weakness.
Tests can detect the toxin in blood, stool, or food samples.
Nerve tests show a pattern different from other nerve diseases.
Imaging or spinal tap may be done to rule out other causes.
Diagnosis is mainly clinical and treatment starts right away.
What is the treatment?
An antitoxin is given immediately to stop the toxin from doing more harm.
Hospital care supports breathing and swallowing if needed.
Patients may need a ventilator until muscle strength returns.
Antibiotics are used for wound infections.
Early treatment greatly improves survival and recovery.
What is the prognosis?
Recovery can take weeks to months as nerves slowly heal.
Most people recover completely with good medical care.
Early antitoxin use prevents complications.
Breathing problems are the main life-threatening risk.
Once recovered, the illness does not recur.
Brachial Plexopathy
What is it?
Brachial plexopathy is an injury to the network of nerves that controls the shoulder, arm, and hand.
It can cause weakness, numbness, or pain in one arm.
These nerves run from the neck to the arm and can be stretched, compressed, or inflamed.
The problem may affect part or all of the arm depending on the location.
Recovery varies depending on the cause and severity of the injury.
What causes it?
It can occur after trauma, such as a fall, accident, or surgery near the shoulder or chest.
Repetitive strain or radiation treatment can injure the nerve network.
Sometimes it’s caused by inflammation after infection (Parsonage-Turner syndrome).
Cancer pressing on the nerves may also cause it.
Rarely, it happens without a clear reason.
How is it diagnosed?
Doctors check muscle strength, sensation, and reflexes in the arm.
Nerve tests (EMG/NCS) help locate and measure the nerve injury.
MRI scans can show damage, swelling, or tumors affecting the nerves.
Blood tests may help find autoimmune or infection causes.
Diagnosis helps plan treatment and predict recovery.
What is the treatment?
Pain is managed with medicines or short courses of steroids.
Physical and occupational therapy help maintain movement and strength.
Severe injuries may need surgery or nerve grafting.
Underlying causes like tumors or infections are treated directly.
Patience and regular follow-up are important for recovery.
What is the prognosis?
Most people improve gradually over months.
Mild cases often recover fully.
Severe injuries or complete nerve tears may leave some weakness.
Recovery depends on the cause and speed of treatment.
Early therapy helps prevent stiffness and improves function.
Brain Abscess
What is it?
A brain abscess is a pocket of infection and pus inside the brain.
It happens when bacteria or fungi reach the brain and cause inflammation.
The swelling can increase pressure inside the skull.
It is a serious condition needing urgent treatment.
With modern care, most people recover well.
What causes it?
Infections from the ear, sinuses, or teeth can spread to the brain.
Germs can also travel through the bloodstream from other body infections.
Head injuries or surgeries can allow bacteria to enter.
People with weak immune systems are at higher risk.
Common bacteria include Streptococcus and Staphylococcus.
How is it diagnosed?
MRI or CT scans show a round area of infection with swelling.
Doctors look for fever, headache, and weakness on one side.
Blood tests and cultures help identify the germs.
Sometimes, a small needle procedure removes pus for testing.
Other brain conditions are ruled out using scans.
What is the treatment?
Strong intravenous antibiotics are started right away.
Surgery may be needed to drain large or deep abscesses.
Medicines are adjusted once test results identify the infection.
Seizure medicines are given to prevent convulsions.
Hospital monitoring ensures the swelling and infection resolve.
What is the prognosis?
Most patients recover fully with timely treatment.
Some may have mild lingering weakness or seizures.
Delay in treatment can cause serious complications.
Survival rates are now very high due to modern antibiotics.
Early diagnosis gives the best outcome.
Carpal Tunnel Syndrome
What is it?
Carpal tunnel syndrome happens when a nerve in your wrist, called the median nerve, gets squeezed.
This nerve controls feeling in your thumb, index, and middle fingers and helps move your hand.
When it’s under pressure, your hand may feel numb, tingly, or weak.
The symptoms often come on slowly and may feel worse at night.
It’s one of the most common nerve problems affecting the hand.
What causes it?
Repetitive hand and wrist movements—like typing or using tools—can irritate the nerve.
Health conditions such as diabetes, thyroid problems, or arthritis can increase the risk.
Fluid buildup in pregnancy can temporarily compress the nerve.
Injury or swelling in the wrist may make the space too tight for the nerve.
Sometimes, no single cause is found—it’s a combination of strain and anatomy.
How is it diagnosed?
Doctors ask about symptoms like tingling, numbness, and night pain.
A physical exam includes tapping or bending the wrist to reproduce symptoms.
Nerve tests (EMG or nerve conduction studies) check how signals travel through the wrist.
An ultrasound may show swelling around the nerve.
Blood tests might be done to rule out thyroid or sugar-related causes.
What is the treatment?
Wearing a wrist splint—especially at night—helps keep the wrist straight and relieves pressure.
Taking breaks from repetitive hand work is important.
Anti-inflammatory medicines or steroid injections can ease swelling and pain.
If severe, surgery can release pressure on the nerve and prevent long-term damage.
Gentle hand exercises help restore strength and movement after recovery.
What is the prognosis?
Most people get better with simple treatments and rest.
Early diagnosis leads to a quicker and more complete recovery.
If untreated, the hand can become weak and lose coordination.
Surgical results are usually excellent, especially when done early.
Antibodies and immune complexes damage nerve cells.
Blood vessel inflammation reduces blood flow to the brain.
Stress, infections, or medication changes may trigger flares.
The exact reason why lupus targets the brain is unknown.
How is it diagnosed?
Doctors look for lupus symptoms with new neurological changes.
MRI and blood tests help detect inflammation.
Spinal fluid tests may show immune activity.
EEG or nerve tests may be done if seizures occur.
Diagnosis is made by combining lab and imaging findings.
What is the treatment?
Corticosteroids reduce brain inflammation.
Immunosuppressants calm the overactive immune system.
Seizures and mood symptoms are treated with specific drugs.
Supportive therapy helps manage fatigue and cognition.
Regular follow-up helps prevent relapses.
What is the prognosis?
Early treatment improves recovery chances.
Some people recover fully; others may have lingering symptoms.
Relapses can occur if lupus flares again.
Ongoing medication helps prevent damage.
With proper care, long-term outlook is generally good.
Lyme Disease of the Nervous System
What is it?
A nerve and brain infection caused by Lyme disease bacteria.
Spread through the bite of an infected tick.
Can affect the face, arms, legs, or spinal nerves.
Early symptoms may include headache, fatigue, and rash.
If untreated, it can cause nerve pain or weakness.
What causes it?
Caused by the bacterium Borrelia burgdorferi.
Transmitted through deer tick bites.
Infection spreads from the skin to nerves and brain.
More common in wooded or grassy areas.
Delay in treatment increases risk of complications.
How is it diagnosed?
History of tick bite or travel to high-risk areas helps.
Blood tests detect Lyme antibodies.
Spinal fluid may show inflammation if brain is affected.
MRI may rule out other neurological diseases.
Diagnosis is based on clinical and lab findings together.
What is the treatment?
Antibiotics such as doxycycline or ceftriaxone cure the infection.
Treatment lasts 2–4 weeks depending on severity.
Pain and nerve symptoms may take time to improve.
Physical therapy helps with strength and balance.
Early treatment prevents long-term nerve damage.
What is the prognosis?
Most patients recover completely with antibiotics.
Some may have lingering fatigue or pain.
Rarely, chronic symptoms may persist after infection.
Early diagnosis gives the best results.
Preventing tick bites avoids reinfection.
Lymphoma of the Central Nervous System (CNS Lymphoma)
What is it?
A type of cancer that starts in the brain or spinal cord.
It involves white blood cells called lymphocytes.
It can occur alone or spread from other body parts.
Symptoms depend on the tumor’s location in the brain.
Common signs include headaches, weakness, or vision changes.
What causes it?
The exact cause is unknown but involves abnormal immune cell growth.
People with weakened immune systems are more at risk.
HIV/AIDS, organ transplants, or immune-suppressing drugs can trigger it.
Genetic and environmental factors may play a role.
It is not contagious.
How is it diagnosed?
MRI or CT scans show the brain lesion.
A biopsy confirms lymphoma under a microscope.
Blood and spinal fluid tests detect abnormal cells.
Eye exams may reveal lymphoma involvement.
Diagnosis requires collaboration between neurology and oncology teams.
What is the treatment?
High-dose chemotherapy is the main treatment.
Radiation therapy may be added for better control.
Steroids can temporarily reduce swelling and symptoms.
Targeted and immunotherapies are improving outcomes.
Supportive care manages fatigue and neurological issues.
What is the prognosis?
Many patients respond well to modern treatment.
Relapse can occur, but new drugs offer better survival.
Early detection improves chances of recovery.
Long-term follow-up helps monitor recurrence.
Some may experience mild lasting neurological effects.
Medial Medullary Syndrome
What is it?
Medial medullary syndrome is a rare type of stroke that affects the lower part of the brainstem, called the medulla.
The medulla controls important functions like movement, sensation, and tongue motion.
When blood flow to this area is blocked, certain nerve pathways stop working properly.
This can cause weakness or paralysis on one side of the body and problems with speech or swallowing.
It is sometimes called Dejerine syndrome, named after the doctor who first described it.
What causes it?
The most common cause is a blockage in a small artery called the anterior spinal artery.
This artery supplies blood to the middle portion of the medulla in the brainstem.
Conditions such as high blood pressure, diabetes, and smoking increase the risk of this kind of stroke.
Less commonly, it can be caused by a blood clot traveling from the heart or neck arteries.
Rarely, inflammation or vessel abnormalities can also lead to this syndrome.
How is it diagnosed?
Doctors usually suspect the diagnosis based on symptoms like one-sided weakness and tongue deviation.
A brain MRI, especially with diffusion-weighted imaging, confirms the diagnosis.
The scan typically shows an area of damage in the medial part of the medulla.
Additional tests like CT angiography can check for blocked or narrowed arteries.
Blood tests and heart studies may be done to look for stroke risk factors or sources of clots.
What is the treatment?
Treatment depends on how quickly the stroke is recognized.
If diagnosed early, clot-busting medications may be used to restore blood flow.
Long-term treatment includes blood thinners, blood pressure control, and stopping smoking.
Physical, occupational, and speech therapy help improve strength and communication.
Ongoing follow-up with a neurologist is important to prevent future strokes.
What is the prognosis?
Recovery varies depending on the size and severity of the stroke.
Many people regain strength and function with early rehabilitation.
Some patients may continue to have speech or swallowing difficulties.
Preventing another stroke through medication and lifestyle changes greatly improves outcomes.
With proper care and therapy, most people can lead meaningful, active lives.
MELAS (Mitochondrial Encephalomyopathy, Lactic Acidosis, and Stroke-like Episodes)
What is it?
MELAS is a rare inherited disorder that affects how the body’s cells produce energy.
It mainly impacts the brain and muscles, causing stroke-like symptoms and weakness.
The name comes from its key features: muscle disease, brain problems, and lactic acid buildup.
People often have repeated episodes that look like strokes but are not caused by blocked blood flow.
Symptoms usually appear in childhood or early adulthood.
What causes it?
MELAS happens because of changes in mitochondrial DNA passed down from the mother.
These changes stop the body from making enough energy for cells to work properly.
The brain, muscles, and heart are most affected because they need the most energy.
Low energy causes cells to switch to less efficient ways of making fuel, leading to lactic acid buildup.
Stress, illness, or fasting can trigger or worsen episodes.
How is it diagnosed?
Doctors use a combination of symptoms, blood tests, and imaging to make the diagnosis.
MRI scans show stroke-like areas not limited to blood vessel regions.
Blood or spinal fluid tests often reveal high lactic acid levels.
A muscle biopsy may show abnormal “ragged red fibers.”
Genetic testing confirms a mitochondrial DNA mutation.
What is the treatment?
There is no cure, but treatment helps control symptoms and prevent complications.
Intravenous L-arginine or citrulline can help during stroke-like episodes.
Anti-seizure medicines are used carefully; valproic acid should be avoided.
Supplements like coenzyme Q10, riboflavin, or L-carnitine may support energy production.
Good nutrition, rest, and avoiding stress or dehydration can help reduce attacks.
What is the prognosis?
The outlook varies depending on the severity and age at onset.
Some people have mild symptoms for years; others develop severe disabilities.
Regular care helps manage symptoms and improve quality of life.
Over time, neurological and muscle problems may gradually worsen.
With supportive treatment, many live for decades after diagnosis.
Meningioma
What is it?
A meningioma is a tumor that grows from the layers covering the brain and spinal cord.
Most are noncancerous and grow slowly over many years.
They may not cause symptoms until they become large.
Some are found by accident during scans for other reasons.
Rarely, they can grow quickly or come back after removal.
What causes it?
The exact cause is unknown, but certain risk factors are known.
It can occur after exposure to radiation, especially during childhood.
Hormones may play a role since it is more common in women.
People with a genetic condition called NF2 are at higher risk.
In most cases, there is no clear trigger or family history.
How is it diagnosed?
Brain MRI is the best way to detect a meningioma.
The tumor usually appears attached to the brain’s covering with a “dural tail.”
CT scans can help identify any bone changes or calcification.
A biopsy confirms the diagnosis after surgical removal.
Regular scans may be done to check for growth over time.
What is the treatment?
Small, symptom-free tumors may just be watched with yearly scans.
Surgery is often curative if the tumor can be safely removed.
Radiation therapy helps when the tumor cannot be fully removed.
Medications may relieve swelling and other symptoms.
Follow-up care includes regular imaging to detect recurrence.
What is the prognosis?
Most meningiomas are benign and curable with surgery.
The risk of recurrence is low for completely removed tumors.
Regular checkups help detect early regrowth if it occurs.
Recovery depends on tumor size and its location in the brain.
Many patients return to normal life after treatment.
Meningitis
What is it?
Meningitis is an infection of the layers covering the brain and spinal cord.
It causes swelling that can lead to headache, fever, and confusion.
It may be caused by bacteria, viruses, or, rarely, fungi.
Bacterial meningitis is serious and can be life-threatening.
Viral meningitis is more common and usually mild.
What causes it?
Bacteria or viruses spread through droplets, saliva, or blood.
The infection can reach the brain from nearby areas like the sinuses or ears.
Sometimes it follows surgery, injury, or weakened immunity.
Certain bacteria like meningococcus or pneumococcus are common causes.
Vaccination has greatly reduced many types of bacterial meningitis.
How is it diagnosed?
Doctors use symptoms like fever, stiff neck, and sensitivity to light as clues.
A lumbar puncture (spinal tap) checks the spinal fluid for infection.
Blood tests and cultures help find the exact germ.
CT or MRI scans may be done to rule out other problems.
Quick diagnosis is vital to start treatment early.
What is the treatment?
Bacterial meningitis needs urgent antibiotics and hospital care.
Steroids may reduce brain swelling and complications.
Antiviral drugs are used if a virus is the cause.
Supportive care includes fluids, pain control, and seizure treatment.
Close contacts may need preventive antibiotics in meningococcal cases.
What is the prognosis?
With early treatment, many people recover fully.
Some may have hearing loss or neurological issues afterward.
Viral meningitis usually resolves without lasting effects.
Delay in treatment can lead to serious complications or death.
Vaccination and awareness are key to prevention.
Meralgia Paresthetica
What is it?
Meralgia paresthetica is a condition that causes tingling, burning, or numbness on the outer part of the thigh.
It happens when a nerve called the lateral femoral cutaneous nerve gets squeezed or irritated.
The nerve only affects sensation, so muscle strength stays normal.
It is more common in people who are overweight or wear tight belts or clothing.
The condition is not dangerous and usually improves with simple lifestyle changes.
What causes it?
The nerve that supplies feeling to the thigh can get trapped under the groin ligament near the hip bone.
Tight clothing, heavy belts, or obesity can put pressure on the nerve.
Pregnancy or recent weight gain can also cause compression.
In some people, diabetes or scar tissue after surgery can make the nerve more sensitive.
Standing or walking for long periods can make symptoms worse.
How is it diagnosed?
Doctors diagnose it mainly by listening to your symptoms and doing a simple exam.
The numbness is limited to the outer thigh and does not affect strength.
Tests like nerve studies or imaging are rarely needed.
A local anesthetic injection that relieves symptoms can confirm the diagnosis.
Other causes like back problems or hip issues are ruled out if needed.
What is the treatment?
Most people get better by avoiding tight belts or clothing and losing weight if needed.
Over-the-counter pain medicines or nerve pain drugs may help.
Injections with numbing medicine or steroids can reduce pain.
Physical therapy or gentle stretching can relieve tension around the hip.
Surgery is rarely needed, only for long-lasting or severe cases.
What is the prognosis?
Most cases improve within a few weeks or months.
Permanent damage or disability is very rare.
Avoiding pressure around the hip helps prevent recurrence.
Even if symptoms come back, they usually respond to the same treatments.
Overall, the outlook is excellent for full recovery.
MGUS-Associated Neuropathy
What is it
MGUS-associated neuropathy is a nerve problem that happens in some people who have a blood condition called Monoclonal Gammopathy of Undetermined Significance (MGUS).
In MGUS, the body makes an extra protein (called an antibody) that is not harmful by itself but can sometimes affect the nerves.
The nerves that carry signals between the brain, spinal cord, and body can become damaged.
This nerve damage causes symptoms like numbness, tingling, or weakness, usually starting in the feet and legs.
MGUS itself is not cancer, but it can rarely change into more serious blood diseases over time.
What causes it
MGUS happens when certain white blood cells make too much of a single antibody protein.
This extra protein can sometimes attach to nerve tissues and cause irritation or damage.
In some cases, the immune system mistakenly attacks the body’s own nerves.
The damage may cause the nerves to lose their protective covering (myelin), slowing or blocking signals.
Doctors don’t fully know why this happens in some people with MGUS and not others.
How is it diagnosed?
Your doctor will ask about your symptoms and do a careful nerve and muscle exam.
Blood tests are done to look for the extra antibody protein that confirms MGUS.
Nerve tests (called nerve conduction studies) check how well the nerves send signals.
Sometimes, other blood or urine tests are done to rule out diabetes, vitamin problems, or other causes.
Rarely, a small sample of nerve tissue (nerve biopsy) may be needed for diagnosis.
What is the treatment?
There is no single cure, but treatments can help reduce symptoms and slow nerve damage.
Medicines like IV immunoglobulin (IVIg) or rituximab can calm the immune system in some patients.
Pain medicines can help control burning or tingling sensations.
Physical therapy helps improve balance and strength.
Regular follow-up visits are important to make sure the condition stays stable.
What is the prognosis?
Many people have mild symptoms that progress slowly over years.
Early diagnosis and treatment can help maintain walking ability and quality of life.
Some people may experience gradual worsening, especially if the IgM type of MGUS is present.
Most patients do not develop serious nerve damage or cancer.
With proper care and monitoring, people with MGUS-associated neuropathy can lead active, independent lives.
Migraine
What is it?
Migraine is a type of recurring headache that can cause severe pain, often on one side of the head.
It is often accompanied by nausea, vomiting, and sensitivity to light or sound.
Some people experience warning signs called “aura,” such as flashing lights or tingling sensations.
Attacks can last from a few hours to a few days.
It is a long-term condition but can be managed with proper treatment and lifestyle adjustments.
What causes it?
Migraine is thought to be caused by overactivity of certain brain pathways and blood vessels.
Changes in brain chemicals, especially serotonin, may play a role.
Hormonal changes, such as during menstruation, can trigger attacks.
Stress, poor sleep, certain foods, or skipping meals are common triggers.
A family history of migraine increases the likelihood of developing it.
How is it diagnosed?
The diagnosis is made based on your symptoms and history of repeated attacks.
No single test confirms migraine, but your doctor may do scans to rule out other causes.
Typical features include throbbing pain, light sensitivity, and nausea.
People with aura often see zigzag lines, flashing lights, or lose part of their vision before pain starts.
Keeping a headache diary helps track triggers and response to treatment.
What is the treatment?
Mild attacks can be treated with rest and over-the-counter pain relievers.
Stronger medicines called triptans are used for more severe episodes.
Preventive medications, such as beta-blockers or anti-seizure drugs, may reduce attack frequency.
Avoiding triggers, staying hydrated, regular meals, and good sleep help prevent headaches.
Some people benefit from stress reduction, relaxation therapy, or physical exercise.
What is the prognosis?
Migraine is a long-term condition but not life-threatening.
Many people see improvement with treatment and lifestyle control.
RCVS is a condition where brain blood vessels suddenly narrow and then return to normal.
It causes sudden, severe “thunderclap” headaches that can be very painful.
It may happen repeatedly over days or weeks.
It can sometimes lead to small strokes or bleeding in the brain.
Despite the dramatic symptoms, it usually resolves completely within weeks.
What causes it?
The exact cause is unclear but involves temporary overactivity of blood vessel control.
Triggers include stress, certain drugs (like antidepressants or migraine medicines), and childbirth.
The condition may also follow exertion, sexual activity, or emotional upset.
Hormonal changes and blood pressure spikes can contribute.
It is not due to permanent damage but to temporary vessel spasm.
How is it diagnosed?
CT or MRI scans help rule out bleeding or stroke.
Angiography shows narrowing of brain arteries that later improves.
The headaches are sudden and reach peak intensity within a minute.
Repeat imaging after a few weeks confirms reversibility.
Other conditions like brain inflammation or aneurysm must be ruled out.
What is the treatment?
Treatment focuses on relieving pain and preventing complications.
Calcium channel blockers (like nimodipine) are often used to relax blood vessels.
Triggers such as certain medications or drugs should be stopped.
Blood pressure is carefully managed to avoid stroke.
Most people recover without long-term treatment.
What is the prognosis?
Most patients recover fully within 1 to 3 months.
Early diagnosis helps prevent complications.
A few may experience small strokes or minor bleeding, but these often heal well.
Recurrence is rare if triggers are avoided.
Long-term outlook is excellent for most people.
Sarcoidosis of the nervous system
What is it?
Neurosarcoidosis is a rare form of sarcoidosis where the body’s defense system attacks parts of the brain, spinal cord, or nerves.
It happens when clusters of immune cells, called granulomas, form in nervous tissue.
These granulomas can irritate or damage nerves, causing weakness, facial drooping, or vision problems.
Sometimes, it also affects the meninges (the brain’s covering), causing headaches or confusion.
It can occur with other symptoms of sarcoidosis, such as cough or fatigue, or sometimes as the first sign of the disease.
What causes it?
The exact cause is unknown, but it’s linked to an overactive immune response.
The immune system reacts to an unknown substance, forming small clusters of inflammation (granulomas).
Genetics and environmental exposure may increase risk.
People with sarcoidosis in other organs, like the lungs or skin, are more likely to develop nervous system involvement.
It is more common among African Americans and women between 20 and 50 years old.
How is it diagnosed?
Diagnosis involves MRI scans to look for inflammation in the brain or nerves.
A lumbar puncture (spinal tap) may show high protein and white cells in the spinal fluid.
Blood tests and chest X-rays check for signs of sarcoidosis in other organs.
A biopsy showing granulomas confirms the diagnosis.
Other diseases like infections or multiple sclerosis are ruled out first.
What is the treatment?
Corticosteroids like prednisone are the main treatment to reduce inflammation.
If symptoms return or are severe, other medicines like methotrexate or azathioprine may be added.
Biologic drugs such as infliximab may be used for resistant cases.
Treatment also includes managing specific symptoms, like seizures or hormone imbalance.
Regular MRI scans help monitor response and prevent relapses.
What is the prognosis?
Many patients improve with treatment, especially when started early.
Some people may have relapses requiring long-term medication.
Persistent inflammation can lead to lasting nerve damage in severe cases.
Regular monitoring helps prevent complications and detect recurrence early.
With proper care, most patients lead full, active lives.
Serotonin Syndrome
## What is it?
Serotonin syndrome is a reaction that happens when the brain has too much serotonin.
It can occur when certain medications are taken together or in high doses.
Symptoms include restlessness, confusion, tremors, and fever.
It can develop quickly—often within hours of taking a new drug or changing a dose.
Severe cases can be life-threatening if not treated promptly.
What causes it?
It’s caused by excessive serotonin activity in the brain and body.
Common triggers include antidepressants (SSRIs, SNRIs), MAO inhibitors, and some pain or migraine medicines.
Combining these drugs or taking too high a dose increases the risk.
Some antibiotics (like linezolid) and recreational drugs (like MDMA) can also trigger it.
The reaction overstimulates nerves that control mood, movement, and body temperature.
How is it diagnosed?
Doctors diagnose it based on symptoms and medication history.
Key signs include tremor, muscle jerks (clonus), sweating, and high temperature.
Blood tests may show muscle breakdown or dehydration but are not specific.
Imaging or spinal fluid tests are usually normal and help rule out other causes.
The “Hunter Criteria” are often used to confirm the diagnosis.
What is the treatment?
The first step is stopping all serotonin-related medications.
Supportive care includes cooling, IV fluids, and calming medicines like benzodiazepines.
A medicine called cyproheptadine may be used to block serotonin’s effects.
Severe cases may require hospital monitoring and muscle relaxation.
Most people improve within one to three days after stopping the drugs.
What is the prognosis?
Most patients recover completely with early treatment.
Severe cases can cause complications like high fever or muscle breakdown but are reversible.
Quick recognition and treatment are key to recovery.
Avoiding dangerous drug combinations prevents recurrence.
Education about medication safety is very important for future prevention.
Sjögren’s Syndrome and the Nervous System
What is it?
Sjögren’s syndrome is an autoimmune disease where the body attacks its moisture-producing glands.
It causes dry eyes, dry mouth, and sometimes nerve problems.
Nerve involvement can lead to numbness, tingling, or burning in the hands and feet.
It can also cause facial weakness, dizziness, or memory problems.
Both the central and peripheral nervous systems can be affected.
What causes it?
It happens when the immune system attacks healthy cells by mistake.
The glands that produce tears and saliva are the first to be affected.
In some people, the immune attack also targets nerves.
This may damage the nerve covering (myelin) or the nerve itself.
Genetic and environmental factors play a role in who develops it.
How is it diagnosed?
Diagnosis is based on symptoms like dry eyes and dry mouth, plus blood and nerve tests.
Blood tests look for antibodies called anti-Ro (SSA) and anti-La (SSB).
A small lip biopsy can confirm the disease by showing immune cell clusters.
Nerve tests (EMG, nerve conduction) detect nerve injury or slowing.
MRI may be used if the brain or spinal cord is involved.
What is the treatment?
Treatment aims to control inflammation and relieve symptoms.
Artificial tears and saliva substitutes help dryness.
Medications like steroids, hydroxychloroquine, or immunosuppressants reduce immune activity.
Pain-relieving drugs such as gabapentin or duloxetine help with burning or tingling.
Severe nerve or brain involvement may need stronger medicines like rituximab.
What is the prognosis?
Many people live well with proper treatment and follow-up.
Nerve symptoms may improve slowly and sometimes do not fully recover.
Regular checkups help detect relapses or complications early.
Long-term inflammation increases the risk of lymphoma, so ongoing monitoring is vital.
With good care, most patients maintain an active and independent life.
Small Fiber Neuropathy
What is it?
Small fiber neuropathy (SFN) is a condition where the small nerves that carry pain, temperature, and automatic body signals are damaged.
These nerves include thinly myelinated A\(\delta\) and unmyelinated C fibers.
People often feel burning, tingling, or sharp pain in the feet and hands, especially at night.
It may also affect automatic body functions like sweating, digestion, or blood pressure.
Muscle strength and reflexes usually stay normal, which helps distinguish it from other neuropathies.
What causes it?
Diabetes and impaired glucose tolerance are the most common causes.
Other causes include autoimmune diseases, infections (like HIV or hepatitis C), certain medications, and toxins.
Some people have inherited forms caused by sodium channel gene mutations (e.g., SCN9A, SCN10A).
In up to half of all cases, no clear cause is found (idiopathic SFN).
Chronic inflammation, oxidative stress, and reduced blood supply to nerves contribute to the damage.
How is it diagnosed?
Diagnosis begins with symptoms such as burning pain, tingling, or temperature changes.
Nerve conduction studies are often normal because large nerves are not affected.
A skin biopsy is the gold standard test, showing reduced intraepidermal nerve fiber density.
Other tests include quantitative sensory testing (QST) and autonomic function studies.
Blood tests look for underlying causes like diabetes, autoimmune markers, or vitamin deficiencies.
What is the treatment?
Treating the underlying cause is most important, such as controlling blood sugar in diabetes.
Medications for nerve pain include gabapentin, pregabalin, duloxetine, or amitriptyline.
Topical treatments such as capsaicin or lidocaine patches may help localized pain.
Autonomic symptoms can be managed with fluids, compression stockings, or medicines like midodrine.
Regular follow-up helps monitor symptoms and adjust treatment as needed.
What is the prognosis?
Many patients improve or stabilize with proper treatment.
Pain may persist but can be controlled in most cases.
Identifying and treating the cause early improves outcomes.
Idiopathic cases can be chronic but are usually not life-threatening.
Long-term follow-up ensures symptom control and quality of life.
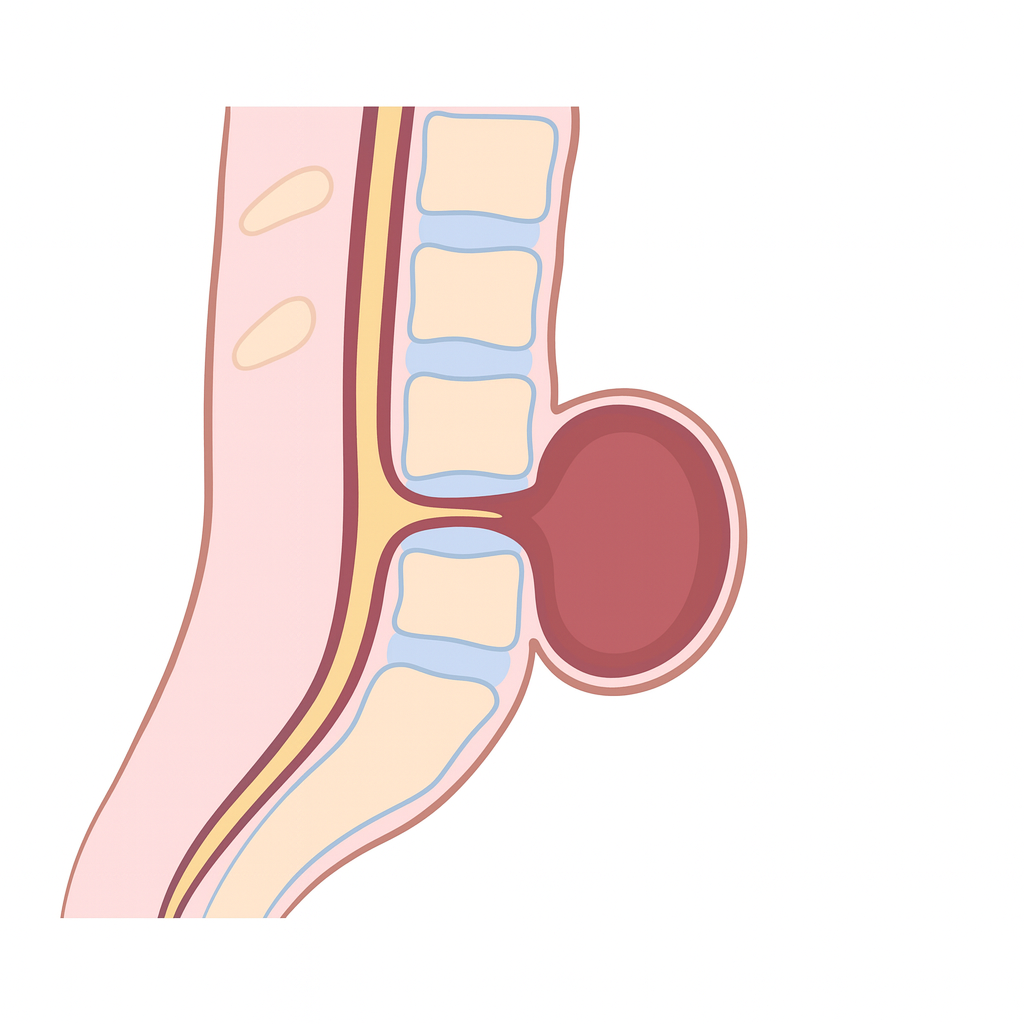
Spina Bifida
What is it?
Spina bifida is a birth defect where the spine and spinal cord do not close properly during early pregnancy.
It is part of a group of conditions called neural tube defects (NTDs).
In severe cases, the spinal cord and its coverings protrude through an opening in the back.
It can cause weakness, paralysis, or bladder and bowel problems.
The most common and serious type is called myelomeningocele.
What causes it?
It occurs when the neural tube fails to close during the 3rd to 4th week of pregnancy.
Low folic acid levels before or during early pregnancy are a major risk factor.
Other risk factors include certain anti-seizure drugs, diabetes, obesity, and high fever in early pregnancy.
Genetics also play a role, and families with one affected child have a higher risk in future pregnancies.
Environmental and nutritional factors can influence the likelihood of occurrence.
How is it diagnosed?
During pregnancy, blood tests can detect high alpha-fetoprotein (AFP) levels.
Ultrasound scans can show spinal defects or protrusions by 18–20 weeks.
Amniocentesis may show increased acetylcholinesterase activity.
After birth, physical examination and imaging like MRI confirm the diagnosis.
Genetic counseling may be recommended if other abnormalities are seen.
What is the treatment?
Early surgery after birth helps close the defect and prevent infection.
Some cases can be treated with prenatal (in utero) surgery before delivery.
Ongoing care includes physical therapy, urology support, and orthopedic management.
Children may need assistive devices for walking and programs for bladder and bowel care.
Folic acid supplements before and during pregnancy can prevent most cases.
What is the prognosis?
Many children live fulfilling lives with proper treatment and rehabilitation.
The level of the spinal defect determines how much movement or sensation is affected.
Early surgery and multidisciplinary care improve long-term outcomes.
Some may develop hydrocephalus requiring a shunt to drain excess brain fluid.
Lifelong follow-up ensures mobility, continence, and independence.
Spinal Cord Injury
What is it?
A spinal cord injury (SCI) happens when the spinal cord is damaged by trauma or disease.
It can cause partial or complete loss of movement and sensation below the level of injury.
Common causes include vehicle accidents, falls, sports injuries, or violence.
The injury may also affect bladder, bowel, and blood pressure control.
Depending on where the injury occurs, it may cause paraplegia (legs only) or quadriplegia (arms and legs).
What causes it?
Most SCIs are caused by trauma that fractures or dislocates the spine.
Other causes include tumors, infections, bleeding, or inflammation around the spinal cord.
The initial mechanical injury is followed by secondary damage from swelling, poor blood flow, and cell death.
This cascade worsens nerve injury and limits recovery if not treated promptly.
Early stabilization of the spine helps prevent further damage.
How is it diagnosed?
Doctors assess muscle strength, sensation, and reflexes to find the level of injury.
MRI scans show spinal cord compression, swelling, or bleeding.
CT scans help detect bone fractures or dislocations.
The ASIA Impairment Scale is used to grade the severity of injury.
Other tests check bladder, bowel, and autonomic function.
What is the treatment?
Immediate care includes stabilizing the spine and supporting breathing and blood pressure.
Surgery may be needed to decompress the spinal cord and fix fractures.
Rehabilitation starts early to preserve muscle strength and prevent complications.
Medications and physical therapy help manage spasticity and pain.
Long-term care focuses on mobility aids, bladder management, and skin protection.
What is the prognosis?
Recovery depends on the level and completeness of injury.
Partial injuries often have better outcomes than complete injuries.
Rehabilitation and assistive technology can restore independence in many cases.
Complications like infections and pressure ulcers can be prevented with care.
Emotional and social support play a key role in long-term adjustment and quality of life.
Spinal Muscular Atrophy (SMA)
What is it?
Spinal muscular atrophy (SMA) is a genetic condition that causes muscles to weaken and shrink (atrophy) over time.
It occurs because the nerve cells in the spinal cord that control movement (motor neurons) are lost.
The brain remains unaffected, so intelligence and thinking ability are normal.
There are several types depending on the age of onset and severity, from severe infantile forms to mild adult-onset disease.
Without treatment, severe forms can affect breathing and swallowing early in life.
What causes it?
SMA is caused by a defect in the SMN1 gene on chromosome 5.
This gene makes a protein essential for motor neuron survival.
When both SMN1 genes are faulty, motor neurons die and muscles lose function.
A backup gene, SMN2, makes some protein but not enough; having more SMN2 copies usually means milder symptoms.
It is inherited in an autosomal recessive pattern—both parents must carry one defective gene.
How is it diagnosed?
A genetic blood test confirms the diagnosis by detecting deletion or mutation of the SMN1 gene.
Doctors may also assess muscle tone, reflexes, and movement abilities.
Nerve and muscle tests (EMG or nerve conduction studies) can show reduced motor neuron activity.
Muscle biopsy is rarely needed today since genetic testing is highly accurate.
Many countries now include SMA in newborn screening programs, allowing early diagnosis before symptoms appear.
What is the treatment?
New treatments can dramatically improve survival and muscle function if started early.
Nusinersen (Spinraza) helps the body make more SMN protein from the SMN2 gene.
Onasemnogene abeparvovec (Zolgensma) replaces the missing SMN1 gene through gene therapy.
Risdiplam (Evrysdi) is an oral medicine that also increases SMN protein production.
Supportive care includes physiotherapy, breathing support, nutrition management, and orthopedic care for posture and scoliosis.
What is the prognosis?
With modern therapies, many children with SMA live longer and gain motor skills previously thought impossible.
Early diagnosis and treatment are key for the best outcomes.
Ongoing physiotherapy helps maintain mobility and joint flexibility.
Severe forms may still need respiratory and feeding support.
With comprehensive care, most patients lead longer, more independent lives than before.
Stiff Person Syndrome (SPS)
What is it?
Stiff Person Syndrome (SPS) is a rare neurological disorder that causes muscle stiffness and painful spasms.
It happens because the body’s immune system attacks parts of the brain and spinal cord that control muscle movement.
The stiffness mainly affects the back and leg muscles, leading to a rigid posture and difficulty walking.
Spasms can be triggered by sudden noise, touch, or emotional stress.
Without treatment, stiffness can worsen and limit daily activities.
What causes it?
SPS is an autoimmune disorder in which the body attacks its own nerve cells.
Most people with SPS have antibodies against an enzyme called GAD65, which helps make GABA—a chemical that calms nerve activity.
Without enough GABA, muscles stay overactive and stiff.
Some cases are linked to cancers (paraneoplastic SPS), especially breast or lung cancer.
It is more common in women and often occurs alongside other autoimmune diseases like diabetes or thyroiditis.
How is it diagnosed?
Diagnosis is based on symptoms, examination, and special tests.
Electromyography (EMG) shows continuous muscle activity even at rest.
A blood test can detect anti-GAD65 or other antibodies related to the disorder.
MRI scans are usually normal but help rule out other causes.
Sometimes doctors look for hidden cancers if a paraneoplastic form is suspected.
What is the treatment?
Medicines that boost GABA levels, like diazepam or baclofen, help relax muscles and reduce stiffness.
Intravenous immunoglobulin (IVIG) or plasmapheresis can reduce harmful antibodies.
Immunosuppressants such as steroids or rituximab may help in more severe or persistent cases.
Physical therapy is vital to improve flexibility, prevent contractures, and support walking.
Treating an underlying cancer (if present) can also improve symptoms.
What is the prognosis?
SPS often improves with treatment, especially when started early.
Many people can manage symptoms and maintain independence with medication and therapy.
Some patients experience relapses, requiring long-term immunotherapy.
Severe cases may affect breathing or cause disability without care.
With proper treatment and support, most patients can live active, fulfilling lives.
Stroke – Cardioembolic
What is it?
A cardioembolic stroke happens when a clot forms in the heart and travels to the brain.
It blocks blood flow suddenly and often causes severe symptoms.
Atrial fibrillation is the most common cause.
The clot travels through arteries and lodges in the brain.
Without urgent treatment, it can lead to permanent brain injury.
What causes it?
This stroke comes from a heart-origin clot that reaches the brain.
Atrial fibrillation allows blood to pool and form clots.
Heart attacks, heart failure, or weak heart muscle increase risk.
Damaged or artificial valves can also form clots.
Infection or a PFO can let clots enter brain circulation.
How is it diagnosed?
A CT or MRI scan confirms the stroke and location.
Echocardiography looks for clots or heart wall problems.
Heart rhythm tests help detect atrial fibrillation.
Blood tests check clotting and other contributing issues.
Vascular imaging can rule out blocked neck or brain arteries.
What is the treatment?
The goal is to restore blood flow quickly.
Clot-dissolving drugs help if given within 4.5 hours.
Thrombectomy can remove clots in large arteries.
Anticoagulants are used afterward to prevent new clots.
Heart conditions and risk factors must be managed.
What is the prognosis?
Outcome depends on severity and treatment timing.
Anticoagulation can reduce recurrence by up to 70%.
Rehabilitation helps with movement and speech recovery.
Some may have lasting weakness or language difficulties.
Regular follow-up helps prevent future strokes.
Stroke - Hemorrhagic
What is it?
Hemorrhagic stroke occurs when a blood vessel in the brain ruptures and bleeds into brain tissue.
The bleeding increases pressure inside the skull and damages surrounding brain cells.
It is less common than ischemic stroke but often more severe.
Symptoms begin suddenly and may include headache, weakness, confusion, or loss of consciousness.
It is a neurological emergency requiring rapid diagnosis and treatment.
What causes it?
The most common cause is long-standing high blood pressure that weakens blood vessel walls.
Cerebral aneurysms can burst and lead to sudden bleeding.
Arteriovenous malformations (AVMs) may rupture and spill blood into the brain.
Blood-thinning medications can increase the risk of bleeding.
Trauma, drug use (such as cocaine), or bleeding disorders may also contribute.
How is it diagnosed?
A non-contrast CT scan quickly identifies bleeding in the brain.
MRI can further define the location and size of the hemorrhage.
CT or MR angiography helps detect aneurysms or vascular malformations.
Blood tests check clotting status, platelet count, and overall health.
Monitoring vital signs and neurological status helps guide treatment decisions.
What is the treatment?
Emergency care focuses on controlling blood pressure and stabilizing the patient.
Surgery may be needed to remove large clots or relieve pressure.
Endovascular procedures can repair aneurysms or AVMs.
Reversal of blood thinners or clotting support may be required.
Intensive care monitoring is essential to prevent complications like swelling or rebleeding.
What is the prognosis?
Outcomes vary based on the size and location of the bleed and speed of treatment.
Some patients recover well with rehabilitation, especially if treated early.
Others may have lasting weakness, speech problems, or cognitive changes.
Mortality is higher than with ischemic stroke, especially in older patients.
Long-term management includes blood pressure control and stroke prevention strategies.
Stroke – Large Vessel Occlusion (LVO)
What is it?
A large vessel occlusion (LVO) stroke happens when a major artery supplying the brain becomes blocked.
This prevents oxygen-rich blood from reaching large areas of the brain.
Symptoms often start suddenly and are usually severe.
Common signs include weakness, speech problems, facial droop, or loss of vision.
It is a medical emergency that requires rapid treatment.
What causes it?
Most LVO strokes are caused by a blood clot traveling from the heart or neck arteries.
Atrial fibrillation is a common source of clots that lead to LVO.
Atherosclerosis (plaque buildup) can also cause blockages.
Rarely, trauma, artery tears, or blood disorders may be involved.
High blood pressure, diabetes, and smoking increase the risk.
How is it diagnosed?
A CT scan or MRI confirms the presence of a stroke.
CT or MR angiography shows which artery is blocked.
Stroke scales help quickly identify severe symptoms.
Blood tests look for contributing conditions or risk factors.
Rapid diagnosis is critical to decide on emergency treatment.
What is the treatment?
A clot-busting drug (tPA) may be given if the patient arrives early.
Mechanical thrombectomy removes the clot using a device threaded through the artery.
This is the most effective treatment for LVO and works up to 24 hours in select cases.
Blood pressure, cholesterol, and glucose are controlled to protect the brain.
Long-term treatment includes blood thinners or stroke prevention medications.
What is the prognosis?
Early thrombectomy greatly improves the chance of recovery.
Without treatment, LVO strokes often cause severe disability.
Many patients regain strength and speech with rehabilitation.
Some may still have weakness, speech problems, or cognitive changes.
Ongoing medical care helps prevent future strokes.
Stroke - Small Vessel (Lacunar Stroke)
What is it?
A small vessel or lacunar stroke occurs when one of the tiny arteries deep inside the brain becomes blocked.
These small strokes usually affect structures like the internal capsule, thalamus, or brainstem.
They are often mild but can still cause weakness, speech changes, or balance problems.
Because they affect small areas, symptoms may be limited but can add up over time if multiple strokes occur.
It is one of the most common types of ischemic stroke, especially in people with long-standing high blood pressure or diabetes.
What causes it?
Small vessel strokes are caused by damage to the tiny penetrating arteries in the brain.
The most common reason is long-term high blood pressure, which weakens and thickens the walls of these vessels.
Diabetes also contributes by damaging the blood vessel lining.
Over time, these changes cause narrowing (lipohyalinosis) and blockage of blood flow.
Less often, small cholesterol plaques or microemboli from larger arteries can block these small vessels.
How is it diagnosed?
Diagnosis is based on symptoms, imaging, and exclusion of other stroke types.
MRI, especially diffusion-weighted imaging (DWI), is the best test—it shows small, deep infarcts usually less than 15 mm wide.
CT scans may appear normal early but can show small areas of damage later.
Vascular imaging (CT or MR angiography) rules out blockages in larger arteries.
Cardiac studies and blood tests help ensure there is no heart-related or clotting cause.
What is the treatment?
Immediate care follows standard ischemic stroke management, including evaluation for clot-busting therapy if eligible.
Antiplatelet drugs (such as aspirin or clopidogrel) are used to prevent future strokes.
Blood pressure control is the most important step in preventing recurrence.
Good management of diabetes, cholesterol, and lifestyle factors—like quitting smoking and regular exercise—helps protect brain blood vessels.
Rehabilitation, including physiotherapy and speech therapy, promotes recovery from weakness or speech problems.
What is the prognosis?
Most people recover well, especially if only one small vessel is affected.
However, repeated small strokes can cause problems with walking, balance, or memory over time.
Strict control of blood pressure and diabetes greatly reduces the risk of future events.
Some patients may develop “vascular dementia” if many small strokes occur over years.
Early diagnosis, lifestyle changes, and medication adherence lead to the best long-term outcome.
Subarachnoid Hemorrhage
What is it?
Subarachnoid hemorrhage (SAH) is bleeding into the space between the arachnoid and pia mater that surrounds the brain.
It causes sudden increase in intracranial pressure and irritation of the meninges.
The hallmark symptom is a sudden, severe “thunderclap” headache, often described as “the worst headache of life.”
Nausea, vomiting, neck stiffness, and brief loss of consciousness may occur.
SAH is a neurological emergency that requires immediate recognition and management.
What causes it?
The most common cause is rupture of a berry (saccular) aneurysm, usually in the circle of Willis.
Other causes include arteriovenous malformations (AVMs), trauma, vasculitis, and coagulation disorders.
In some patients, no source of bleeding is found, termed perimesencephalic SAH, which usually has a better prognosis.
Risk factors include hypertension, smoking, family history of aneurysms, and certain genetic disorders (e.g., polycystic kidney disease).
Cocaine or amphetamine use can acutely raise blood pressure and precipitate rupture.
How is it diagnosed?
Non-contrast CT scan of the head is the first and most sensitive test in the first 24 hours.
If CT is negative but suspicion remains high, lumbar puncture is performed to look for xanthochromia (yellow discoloration from hemoglobin breakdown).
CT or MR angiography identifies the aneurysm or vascular malformation responsible.
Digital subtraction angiography (DSA) remains the gold standard for detailed vascular imaging.
Blood tests and ECG are often performed to assess for associated electrolyte disturbances and cardiac stress.
What is the treatment?
Immediate stabilization of airway, breathing, and circulation is essential.
Blood pressure control is crucial—avoid extreme hypertension but maintain cerebral perfusion.
Definitive management involves securing the aneurysm, either by surgical clipping or endovascular coiling.
Nimodipine, a calcium channel blocker, is given to prevent delayed cerebral vasospasm.
Patients require monitoring in a neurocritical care unit for complications such as rebleeding, hydrocephalus, and seizures.
What is the prognosis?
Outcome depends on the severity at presentation, often graded by the Hunt and Hess scale or WFNS scale.
Mortality is high—about 30–40%, with many survivors experiencing neurological deficits.
Early aneurysm repair and meticulous intensive care improve survival and reduce complications.
Common long-term issues include cognitive impairment, fatigue, and mood disorders.
Prompt diagnosis, aneurysm treatment, and prevention of vasospasm significantly improve prognosis.
Subdural Hemorrhage
What is it?
Subdural hemorrhage (SDH) is bleeding between the dura mater and arachnoid mater of the brain.
It results from tearing of bridging veins that drain from the cerebral cortex to the dural sinuses.
The bleeding causes accumulation of blood in a crescent-shaped pattern along the brain surface.
It can be acute, subacute, or chronic, depending on the time since injury.
SDH can cause brain compression and increased intracranial pressure, leading to neurological deterioration.
What causes it?
The most common cause is head trauma, which may be mild or unnoticed, especially in the elderly.
Cerebral atrophy stretches bridging veins, making them prone to rupture even with minor falls.
Anticoagulant or antiplatelet therapy increases the risk of bleeding and expansion of existing SDH.
Other causes include alcohol abuse, seizures, and coagulopathies.
Rarely, spontaneous SDH can occur from intracranial hypotension or vascular malformations.
How is it diagnosed?
Non-contrast CT scan of the brain is the primary diagnostic test, showing a crescent-shaped collection over the cerebral convexity.
Acute SDH appears hyperdense, subacute becomes isodense, and chronic appears hypodense over time.
MRI can help identify isodense or chronic collections and differentiate SDH from other pathologies.
Mass effect and midline shift indicate severity and guide surgical decision-making.
Coagulation studies and medication history are essential for identifying contributing factors.
What is the treatment?
Surgical evacuation (burr holes or craniotomy) is indicated for large or symptomatic hematomas.
Observation and serial imaging may be appropriate for small, asymptomatic, or chronic cases.
Correction of coagulopathy and cessation of anticoagulants are crucial to prevent rebleeding.
Supportive care includes head elevation, ICP control, and close neurological monitoring.
Chronic SDH often requires drainage and postoperative follow-up to detect recurrence.
What is the prognosis?
Prognosis depends on the size of the hematoma, level of consciousness at presentation, and patient age.
Acute SDH has a high mortality rate, especially in older adults and those with severe trauma.
Chronic SDH generally has a good prognosis if recognized early and treated effectively.
Recurrence is common, particularly in elderly patients or those with residual subdural membranes.
Early diagnosis and surgical intervention significantly improve neurological outcomes.
Suprascapular Palsy
What is it?
Suprascapular palsy is an injury or compression of the suprascapular nerve.
This nerve helps control shoulder lifting and rotation.
It affects the supraspinatus and infraspinatus muscles.
Results in weakness, pain, or limited motion.
Often seen in athletes and people doing overhead work.
What causes it?
Repetitive overhead activities (sports or labor).
Direct shoulder or neck injury.
Compression from a cyst or torn ligament.
Nerve stretching during sudden movement.
Sometimes the cause is unknown.
What are the symptoms?
Dull shoulder pain in the upper or back area.
Weakness lifting or rotating the arm.
Worsening pain with activity.
Shoulder fatigue or limited function.
Muscle thinning in chronic cases.
How is it diagnosed?
Physical exam for weakness and motion limits.
MRI or ultrasound to detect nerve compression.
EMG to test nerve and muscle health.
Nerve conduction tests if needed.
Imaging may also rule out rotator cuff tears.
What is the treatment?
Rest and avoiding painful shoulder positions.
Physical therapy to strengthen and restore motion.
Anti-inflammatory medications as needed.
Treating underlying causes like cysts or tears.
Surgery is rare and reserved for severe cases.
What is the prognosis?
Many people recover fully with therapy.
Recovery usually takes weeks to months.
Early diagnosis improves outcomes.
Long-standing cases may have partial weakness.
Strengthening and posture help prevent recurrence.
Syringomyelia
What is it?
Syringomyelia is a condition where a fluid-filled cavity (called a syrinx) forms inside the spinal cord.
This cavity can slowly get bigger and damage the nerves in the spinal cord.
It often causes problems with feeling, especially pain and temperature, in the arms and hands.
Muscle weakness and wasting, especially in the hands, are common.
Symptoms usually develop slowly over months or years.
What causes it?
The most common cause is a problem at the base of the brain called Chiari malformation, where brain tissue pushes into the spinal canal.
Past injuries to the spine, such as trauma or surgery, can also lead to syringomyelia.
Tumors or growths in the spinal cord may block fluid flow and cause a syrinx to form.
Infections or inflammation around the spinal cord can sometimes be a cause.
In some cases, no clear cause is found (idiopathic syringomyelia).
How is it diagnosed?
Doctors start with a physical exam and ask about symptoms like numbness, weakness, or pain.
MRI (magnetic resonance imaging) of the spine is the main test to see the syrinx and any related problems.
Sometimes, special MRI scans are done to see how spinal fluid flows.
Other tests may be used to look for causes, such as tumors or Chiari malformation.
Nerve and muscle tests (EMG) can help check how the nerves are working.
What is the treatment?
Treatment depends on the cause and how severe the symptoms are.
Surgery may be needed to correct the underlying problem, such as Chiari malformation or to drain the syrinx.
Some people with mild or stable symptoms are monitored with regular MRI scans and checkups.
Physical therapy and pain management can help with muscle weakness and discomfort.
Treating the underlying cause, when possible, can stop the syrinx from getting worse.
What is the prognosis?
Many people see improvement or stabilization of symptoms after treatment, especially if treated early.
Some nerve damage may be permanent if the syrinx has been present for a long time.
Regular follow-up is important to monitor for changes or new symptoms.
Early diagnosis and treatment give the best chance for a good outcome.
With proper care, many patients can lead active and fulfilling lives.
Tardive Dyskinesia
What is it?
Tardive dyskinesia is a condition that causes involuntary, repetitive movements, often of the face, mouth, or limbs.
It usually develops after taking certain medications for a long time, especially those used to treat mental health conditions.
The movements can include lip smacking, tongue movements, grimacing, or rapid blinking.
These movements are not under the person’s control and can be mild or severe.
Tardive dyskinesia can affect daily activities and may be distressing to those who have it.
What causes it?
The main cause is long-term use of medications that block dopamine, a brain chemical involved in movement.
Medicines most commonly linked to tardive dyskinesia include antipsychotics and some drugs for nausea.
The risk increases the longer someone takes these medications and at higher doses.
Older adults and women may be at higher risk.
Sometimes, symptoms can continue even after stopping the medication.
How is it diagnosed?
Diagnosis is based on noticing the typical movements and a history of taking certain medications.
There are no special blood tests or scans needed for diagnosis.
Doctors may use a movement rating scale to track symptoms over time.
Other conditions with similar symptoms may need to be ruled out.
Early recognition is important to help manage the condition.
What is the treatment?
The first step is to review and possibly adjust the medications causing the symptoms.
Sometimes, switching to a different medicine can help reduce the movements.
There are specific medications approved to treat tardive dyskinesia and help control the movements.
Other treatments, like certain muscle relaxants, may be tried if needed.
Regular doctor visits are important to monitor and manage symptoms.
What is the prognosis?
Some people improve after changing or stopping the medication, but symptoms can last a long time.
In some cases, the movements may become less noticeable over time.
For others, the symptoms can be persistent and affect quality of life.
Early detection and treatment can improve outcomes.
Support from healthcare providers, family, and friends can help patients cope with the condition.
Tarsal Tunnel Syndrome
What is it?
Tarsal tunnel syndrome is a condition where a nerve in the ankle gets squeezed or compressed.
This nerve, called the tibial nerve, passes through a narrow space near the inside of the ankle.
Compression can cause pain, tingling, or numbness in the foot and toes.
Symptoms often get worse with standing or walking for long periods.
It is similar to carpal tunnel syndrome but affects the ankle and foot instead of the wrist and hand.
What causes it?
Tarsal tunnel syndrome is usually caused by anything that puts pressure on the tibial nerve.
Causes can include flat feet, swelling, injuries, or growths like cysts near the ankle.
Medical conditions like diabetes or arthritis can increase the risk.
Repetitive activities or standing for long times may contribute.
Sometimes, the cause is not found.
How is it diagnosed?
Doctors ask about symptoms and examine the foot and ankle.
Tapping over the nerve (Tinel’s sign) may cause tingling or pain.
Special nerve tests can show if the nerve is being compressed.
Imaging like ultrasound or MRI may be used to look for causes of compression.
Other foot problems may need to be ruled out before making the diagnosis.
What is the treatment?
Treatment usually starts with rest, changing activities, and wearing supportive shoes or inserts.
Medicines like anti-inflammatories can help reduce pain and swelling.
Physical therapy may help improve symptoms.
In some cases, injections or surgery may be needed if symptoms do not improve.
Treating any underlying cause, such as removing a cyst or controlling diabetes, is important.
What is the prognosis?
Many people improve with simple treatments and activity changes.
If treated early, long-term nerve damage can often be prevented.
Some people may need surgery if symptoms are severe or do not get better.
Recovery after surgery is usually good, but it may take time.
Ongoing support and foot care can help prevent symptoms from returning.
Temporal Arteritis (Giant Cell Arteritis)
What is it?
Temporal arteritis, also called giant cell arteritis, is an inflammation of the blood vessels, mainly those in the head.
It most often affects adults over 50 years old.
The condition can cause headaches, scalp tenderness, and jaw pain.
It may lead to vision problems if not treated quickly.
It is considered a medical emergency because of the risk of permanent vision loss.
What causes it?
The exact cause is not known, but it is thought to involve the immune system attacking blood vessel walls.
Age is a major risk factor, as it mainly affects older adults.
Genetics and environmental factors may play a role.
It may sometimes occur with another condition called polymyalgia rheumatica.
There is no evidence that lifestyle or diet alone causes the disease.
How is it diagnosed?
Doctors diagnose it based on symptoms like headache, jaw pain, and vision changes.
Blood tests can show signs of inflammation, such as a high ESR or CRP.
A biopsy of the temporal artery may be done to confirm the diagnosis.
Imaging tests like ultrasound or MRI can help detect inflamed arteries.
Quick diagnosis is important to prevent vision loss.
What is the treatment?
Treatment usually starts right away with high-dose steroids (like prednisone) to reduce inflammation.
Sometimes, other medicines are added to help lower the steroid dose and control the disease.
Low-dose aspirin may be recommended to reduce the risk of blood clots.
Regular follow-up is needed to monitor symptoms and side effects of treatment.
Treatment may last for a year or longer, with gradual reduction of medication.
What is the prognosis?
Most people respond well to treatment if started early.
Vision loss can be permanent if treatment is delayed.
Some people may have relapses and need longer treatment.
Side effects from steroids are possible, so regular check-ups are important.
With proper care, most people can return to normal activities.
Temporomandibular Joint (TMJ) Syndrome
What is it?
TMJ syndrome is a disorder affecting the jaw joint and the muscles that control jaw movement.
It often causes pain or discomfort in the jaw, face, or around the ear.
People may notice clicking, popping, or grating sounds when opening or closing the mouth.
Jaw stiffness or trouble opening the mouth wide is common.
It can affect one or both sides of the jaw.
What causes it?
TMJ syndrome can be caused by jaw injury or arthritis in the joint.
Teeth grinding or clenching (especially during sleep) can strain the jaw joint.
Stress, which leads to jaw muscle tension, may contribute.
Poor bite alignment or missing teeth can increase risk.
Sometimes, the exact cause is not known.
How is it diagnosed?
Doctors ask about symptoms and examine the jaw for tenderness, movement, and sounds.
They may check how wide you can open your mouth and feel for clicking or popping.
Dental x-rays or other imaging (like MRI) may be used if needed.
Diagnosis is often made based on symptoms and examination alone.
Other causes of facial pain are ruled out before making the diagnosis.
What is the treatment?
Most cases improve with simple measures like rest, a soft diet, and avoiding wide jaw movements.
Applying warm compresses or gentle jaw exercises may help relieve pain.
Medicines such as pain relievers or muscle relaxants can be used if needed.
A dentist may suggest a mouth guard or splint, especially if you grind your teeth.
Surgery is rarely needed and is only considered if other treatments do not help.
What is the prognosis?
Most people get better with simple treatments and time.
Symptoms may come and go, but are usually not serious.
Managing stress and avoiding jaw overuse can help prevent flare-ups.
Long-term problems are uncommon if treated early.
Ongoing dental care and follow-up can help keep symptoms under control.
Thoracic Outlet Syndrome
What is it?
Thoracic outlet syndrome is a condition where nerves or blood vessels are squeezed as they pass from the neck to the arm.
It can cause pain, numbness, tingling, or weakness in the arm or hand.
Some people may notice swelling or color changes in the arm.
Symptoms often get worse with certain arm positions or activities.
There are three main types: nerve, vein, and artery compression, with nerve type being the most common.
What causes it?
It can be caused by extra ribs, tight muscles, or abnormal bands of tissue in the neck or shoulder.
Repetitive overhead movements or injuries can increase the risk.
Poor posture or carrying heavy loads may contribute.
Some people are born with anatomy that makes them more likely to develop this condition.
Sometimes, the exact cause is not found.
How is it diagnosed?
Doctors ask about symptoms and examine the neck, shoulder, and arm.
Certain arm positions or movements during the exam may reproduce symptoms.
Imaging tests like ultrasound, MRI, or nerve studies may be done to look for compression.
Blood flow tests can help if swelling or color changes are present.
Other conditions with similar symptoms are ruled out before diagnosis.
What is the treatment?
Treatment often starts with physical therapy to improve posture and strengthen shoulder muscles.
Avoiding activities that trigger symptoms is important.
Pain relievers or anti-inflammatory medicines may help manage discomfort.
In some cases, surgery is needed to relieve pressure on nerves or blood vessels.
Ongoing care and exercises can help prevent symptoms from returning.
What is the prognosis?
Many people improve with therapy and activity changes.
Early treatment can prevent long-term nerve or blood vessel damage.
Some may need surgery, especially if symptoms are severe or do not improve.
After treatment, most people can return to normal activities.
Regular follow-up helps ensure symptoms stay under control.
Tics
What is it?
Tics are sudden, quick movements or sounds that a person does over and over again.
These movements or sounds are hard to control and may happen many times a day.
Tics can involve blinking, facial grimacing, shoulder shrugging, or making noises like throat clearing.
They often start in childhood, most commonly between ages 4 and 6.
Tics may come and go, and their severity can change over time.
What causes it?
The exact cause of tics is not fully understood, but both genes and environment play a role.
Tics often run in families, suggesting a genetic link.
Stress, excitement, or fatigue can make tics more noticeable or frequent.
Some infections or changes in brain chemicals may also contribute.
Most tics are not caused by anything a child or parent did.
How is it diagnosed?
Doctors diagnose tics by asking about symptoms and watching the movements or sounds.
No special blood tests or scans are usually needed.
The doctor will check how long the tics have been present and how they affect daily life.
It is important to rule out other conditions that may look similar to tics.
Early diagnosis can help families understand and manage tics better.
What is the treatment?
Many children with mild tics do not need treatment, just reassurance and support.
Behavioral therapy, such as habit reversal training, can help children control bothersome tics.
Medicines may be used if tics are severe or interfere with daily activities.
Treating other conditions like ADHD or anxiety can also help improve tics.
Regular follow-up with the doctor helps track symptoms and adjust care as needed.
What is the prognosis?
Most children with tics improve as they get older, and many outgrow them by adolescence.
Tics may come and go, and sometimes return during times of stress.
Some people continue to have tics into adulthood, but they are often milder.
Support from family, teachers, and friends helps children cope with tics.
Early understanding and treatment can lead to better outcomes and less worry.
Tinnitus
What is it?
Tinnitus is the hearing of sounds, such as ringing or buzzing, when there is no external noise present.
The sound may be heard in one or both ears, or inside the head.
It can be constant or come and go, and may be soft or loud.
Many people notice tinnitus more in quiet settings or at night.
Tinnitus is a common problem and can affect people of all ages.
What causes it?
Tinnitus can happen when there is damage to the tiny hair cells in the inner ear, often from loud noise or aging.
Ear infections, earwax buildup, or certain medications can also cause tinnitus.
Conditions like hearing loss, head injuries, or problems with blood vessels may play a role.
Sometimes, stress or anxiety can make tinnitus more noticeable.
In many cases, the exact cause is not found.
How is it diagnosed?
The doctor will ask about your symptoms and medical history.
An ear exam will be done to check for ear problems.
Hearing tests are often used to see if there is any hearing loss.
Sometimes, imaging tests may be needed if the tinnitus is only in one ear or is pulsating.
The doctor may ask about medicines you take or recent illnesses to help find the cause.
What is the treatment?
Treating any underlying ear problems, such as removing wax or treating infections, can help.
Hearing aids may help if you have hearing loss along with tinnitus.
Sound therapy or using background noise can make tinnitus less noticeable.
Counseling or cognitive behavioral therapy can help you cope with the stress or anxiety tinnitus may cause.
Medicines are rarely used, but may help if you have trouble sleeping or feel very anxious.
What is the prognosis?
For many people, tinnitus does not get worse and may improve over time.
Learning ways to manage tinnitus can help reduce its impact on daily life.
Most people can continue normal activities with little or no trouble.
Tinnitus can be bothersome, but serious complications are rare.
Support from healthcare providers, family, and friends can make coping with tinnitus easier.
Tolosa–Hunt Syndrome
What is it?
Tolosa–Hunt Syndrome is a rare cause of sudden, painful eye movement due to inflammation around the eye nerves.
It often causes severe pain behind one eye, followed by weakness or paralysis of the eye muscles.
The pain may spread to nearby areas like the forehead or temple.
The condition affects the area called the cavernous sinus or orbital apex, where many eye nerves pass.
It is not an infection or cancer, but an inflammation that can mimic more serious conditions.
What causes it?
The exact cause is unknown, but it is believed to result from an autoimmune inflammation.
The immune system attacks tissues around the nerves controlling eye movement.
It is not linked to trauma or infection.
Rarely, it may follow or be confused with other conditions like sarcoidosis or vasculitis.
Stress or immune reactions might trigger the inflammation in some individuals.
How is it diagnosed?
Diagnosis is based on symptoms of eye pain and double vision, along with imaging studies.
MRI of the brain and orbit often shows inflammation near the eye nerves.
Blood tests help rule out infections or autoimmune diseases.
Other causes like tumors or aneurysms must be excluded first.
Rapid response to steroids strongly supports the diagnosis.
What is the treatment?
Corticosteroids are the main treatment and usually bring quick relief from pain.
The dose is gradually reduced over weeks to months to prevent relapse.
If symptoms return, another short course of steroids may be needed.
In rare cases, other immune-suppressing medicines may be added.
Pain control and follow-up MRI are important parts of management.
What is the prognosis?
Most people recover completely with proper treatment.
Eye movements and pain usually improve within days to weeks.
Some may experience occasional relapses that respond to steroids.
Permanent eye nerve weakness is uncommon.
Long-term outlook is generally excellent with early recognition and care.
Tourette Syndrome
What is it?
Tourette Syndrome is a condition that causes sudden, repeated movements or sounds called tics.
These can include blinking, shrugging, sniffing, or throat clearing.
Tics often start in childhood and may change over time.
They can get worse with stress and lessen during calm or focused activities.
The condition is not dangerous, but it can affect school or social life.
What causes it?
It results from changes in how the brain controls movement and habits.
The circuits involving dopamine and other brain chemicals are overactive.
Genetics play a major role, and it often runs in families.
Stress, fatigue, or infections may temporarily worsen symptoms.
It is not caused by parenting style or emotional weakness.
How is it diagnosed?
Diagnosis is based on observing tics and their pattern over time.
No specific blood test or scan confirms it.
Doctors look for both motor (movement) and vocal (sound) tics lasting more than a year.
Other conditions like seizures or stereotypies are ruled out.
A neurologist or movement disorder specialist usually makes the diagnosis.
What is the treatment?
Many children need only reassurance and education.
Behavioral therapy such as CBIT can help manage tics.
Medicines like risperidone or clonidine may be used for severe tics.
Treating associated conditions such as ADHD or anxiety is important.
Support from teachers and family improves coping and confidence.
What is the prognosis?
Tics often peak in early adolescence and improve with age.
Many people have fewer or no tics as adults.
Emotional support helps children adapt and thrive.
Recurrences can happen during stress but are usually mild.
Long-term outcomes are excellent for most individuals.
Transient Ischemic Attack (TIA)
What is it?
A Transient Ischemic Attack, or TIA, is often called a “mini-stroke.”
It happens when blood flow to part of the brain is briefly blocked.
Symptoms are similar to a stroke but last only minutes to hours.
Common symptoms include weakness, speech difficulty, or vision loss.
It is a serious warning sign for a future stroke.
What causes it?
TIA occurs due to a temporary blockage in a brain artery, often from a small blood clot.
Risk factors include high blood pressure, diabetes, smoking, and high cholesterol.
Irregular heart rhythms like atrial fibrillation can send clots to the brain.
Narrowing of neck arteries (carotid stenosis) also increases risk.
Poor lifestyle habits and older age make TIAs more likely.
How is it diagnosed?
TIA is diagnosed by evaluating symptoms and doing brain scans.
MRI or CT helps rule out a full stroke or bleeding.
Carotid ultrasound and heart tests identify possible sources of clots.
Blood work checks for cholesterol, sugar, and clotting problems.
Doctors may observe patients briefly, even if symptoms have resolved.
What is the treatment?
Treatment focuses on preventing a future stroke.
Blood thinners like aspirin or clopidogrel are commonly prescribed.
Blood pressure, sugar, and cholesterol control are essential.
Lifestyle changes such as quitting smoking and regular exercise are vital.
Surgery or stenting may be done if neck arteries are severely narrowed.
What is the prognosis?
A TIA is reversible, but it is a major warning sign for stroke.
The highest risk of stroke is within days after a TIA.
Prompt evaluation and treatment greatly reduce this risk.
With proper care, most people recover fully and prevent future events.
Regular follow-up and healthy habits protect long-term brain health.
Transverse Myelitis
What is it?
Transverse myelitis is an inflammation of the spinal cord that causes sudden weakness, numbness, and bladder problems.
It affects both sides of the body below a certain level, depending on where the spinal cord is inflamed.
The condition can come on quickly over hours or days.
It is not an infection but an immune reaction that damages the nerve fibers in the spine.
Early treatment can help prevent long-term disability.
What causes it?
It can occur after viral or bacterial infections that trigger an immune response.
Some cases are linked to autoimmune diseases such as multiple sclerosis or neuromyelitis optica.
In many people, the exact cause is not found.
Rarely, it can happen after vaccination or other immune stimulation.
The inflammation damages the protective myelin around spinal nerves.
How is it diagnosed?
MRI scans show inflammation or swelling within the spinal cord.
A spinal tap (lumbar puncture) checks for infection and immune activity in the fluid.
Blood tests may look for antibodies linked to specific disorders like NMOSD or MOG disease.
Other conditions such as stroke, compression, or tumor are ruled out with imaging.
Doctors assess strength, sensation, and reflexes to localize the spinal level affected.
What is the treatment?
High-dose steroids are given early to reduce inflammation and swelling.
If symptoms do not improve, plasma exchange may be used to remove harmful antibodies.
Some patients may need longer-term immune therapy to prevent relapses.
Physical and occupational therapy help restore movement and independence.
Pain control, bladder training, and support care are key parts of recovery.
What is the prognosis?
Many patients recover well, especially with early treatment.
Some may be left with mild weakness or numbness.
Severe cases can lead to lasting disability or need for mobility aids.
Follow-up is important to monitor for recurrence or conversion to multiple sclerosis.
With rehabilitation and support, most people regain significant function.
Trigeminal Neuralgia
What is it?
Trigeminal neuralgia is a nerve condition that causes sudden, sharp, electric shock-like pain in the face.
It affects one side of the face, usually the cheek or jaw.
Pain can be triggered by light touch, talking, or brushing teeth.
Episodes are brief but can happen many times a day.
It is sometimes called the “suicide disease” because of its intensity, though it can be treated effectively.
What causes it?
The main cause is pressure on the trigeminal nerve by a nearby blood vessel.
This pressure damages the nerve covering (myelin), causing it to misfire.
In some cases, it is related to multiple sclerosis or a tumor pressing on the nerve.
Injury or infection in the face may also play a role.
Often, no clear cause is found, especially in older adults.
How is it diagnosed?
Diagnosis is based on the description of pain—brief, sharp, one-sided, and trigger-sensitive.
The doctor will check the face and nerve function.
MRI scans are done to rule out tumors or multiple sclerosis.
Tests may help confirm nerve compression or exclude dental or sinus problems.
Response to medications like carbamazepine helps confirm the diagnosis.
What is the treatment?
First-line treatment is medication that calms overactive nerves, such as carbamazepine or oxcarbazepine.
If these fail, other drugs like gabapentin or baclofen can be tried.
Surgery may relieve pressure on the nerve (microvascular decompression).
For those who cannot have surgery, procedures like radiosurgery or nerve blocks may help.
Lifestyle changes and stress management can reduce pain triggers.
What is the prognosis?
Many patients respond very well to medication.
Surgical options provide long-lasting relief for most who need them.
Recurrence may happen but can often be controlled again with treatment.
It is not life-threatening, but chronic pain can affect mood and quality of life.
With proper care, most people live normally and pain-free.
Trochlear Nerve (Cranial Nerve IV) Palsy
What is it?
Trochlear nerve palsy is a weakness of one eye muscle that causes double vision.
It affects the superior oblique muscle, which helps the eye move downward and inward.
People often notice vertical double vision, especially when looking down.
To compensate, they may tilt their head to one side.
It can be temporary or permanent, depending on the cause.
What causes it?
The most common cause is small blood vessel damage from diabetes or high blood pressure.
Head injury can stretch or damage the delicate trochlear nerve.
It may also occur with brain tumors, inflammation, or stroke.
Some people are born with it and only notice symptoms later in life.
Rarely, it can follow surgery or infection near the brainstem.
How is it diagnosed?
Eye movement testing helps identify the affected muscle.
The Bielschowsky head tilt test confirms the diagnosis by worsening the double vision on head tilt.
MRI or CT scans may be ordered to rule out trauma or structural causes.
Blood sugar and blood pressure are checked for small-vessel disease.
The doctor examines for signs of other nerve involvement.
What is the treatment?
Many cases recover on their own within a few months.
Prism glasses can reduce double vision during recovery.
Treating underlying problems like diabetes helps prevent recurrence.
Persistent cases may need eye muscle surgery for alignment.
Eye exercises and regular follow-up support visual recovery.
What is the prognosis?
Most people recover fully, especially if the cause is small-vessel disease or mild trauma.
Recovery usually happens within 3–6 months.
Surgery or prism glasses can correct lasting double vision.
Recurrence is uncommon once the cause is treated.
Early diagnosis helps avoid long-term visual strain and discomfort.
Tuberculosis of the Central Nervous System
What is it
Tuberculosis of the central nervous system (CNS-TB) is an infection of the brain or spinal cord caused by Mycobacterium tuberculosis, the same bacteria that cause lung tuberculosis.
It can affect the brain’s protective coverings (meninges), brain tissue itself (tuberculoma), or cause fluid accumulation and swelling.
This condition is serious and can lead to neurological problems if not treated early.
It is more common in areas where tuberculosis is widespread, such as parts of Asia and Africa.
CNS-TB can occur in people of any age but is more frequent in those with weakened immune systems.
What causes it
The infection starts when tuberculosis bacteria spread from the lungs or another part of the body through the bloodstream to the brain.
Once in the brain, the bacteria cause inflammation and the formation of small nodules called tubercles.
These can merge to form larger masses (tuberculomas) or cause meningitis, an inflammation of the brain’s protective layers.
People with HIV, diabetes, or those on long-term steroids are at higher risk of developing CNS-TB.
Poor nutrition, crowded living conditions, and lack of access to medical care also increase susceptibility.
How is it diagnosed?
Doctors suspect CNS-TB when patients have symptoms like fever, headache, vomiting, seizures, or confusion lasting for days or weeks.
Brain imaging such as MRI or CT scans can show characteristic lesions, often appearing as ring-shaped areas.
A spinal tap (lumbar puncture) may be done to test cerebrospinal fluid for signs of infection or tuberculosis bacteria.
Advanced tests like GeneXpert or PCR can help confirm the presence of Mycobacterium tuberculosis DNA.
Blood tests and chest X-rays may be used to look for TB infection in other parts of the body.
What is the treatment?
The main treatment for CNS-TB is a combination of anti-tubercular medications, usually given for 9 to 12 months.
These include isoniazid, rifampicin, pyrazinamide, and ethambutol in the initial phase of therapy.
Corticosteroids may be added to reduce brain swelling and inflammation.
Seizure medications are prescribed if the patient has convulsions.
Regular follow-up and brain scans help monitor the response to treatment and prevent relapse.
What is the prognosis?
The outcome depends on how early the condition is diagnosed and treated.
With timely treatment, many patients recover completely or with minimal neurological problems.
Delay in treatment can lead to permanent complications such as paralysis, vision problems, or cognitive issues.
People with HIV or other immune deficiencies tend to have a poorer prognosis.
Early detection, proper medication, and good nutrition greatly improve chances of recovery.
Ulnar Neuropathy at the Wrist
What is it?
Ulnar neuropathy at the wrist is when the ulnar nerve is compressed near the wrist.
This nerve controls feeling in the ring and little fingers and some hand movements.
Compression causes numbness, tingling, and weakness in the hand.
It is also called Guyon’s canal syndrome.
Symptoms usually affect the hand but not the forearm.
What causes it?
Repeated pressure on the wrist, such as from cycling or using hand tools.
Injuries or swelling near the wrist that press on the nerve.
Growths like cysts or tumors in the wrist area.
Certain wrist positions held for long periods.
Anatomical differences that make the nerve more likely to be compressed.
How is it diagnosed?
Doctors ask about symptoms and examine the hand and wrist.
Nerve conduction studies check how well the nerve sends signals at the wrist.
Electromyography (EMG) looks at the muscles controlled by the nerve.
Imaging tests like ultrasound or MRI can show any cysts or abnormalities.
Diagnosis is based on symptoms, physical exam, and test results.
What is the treatment?
Avoid activities that put pressure on the wrist or cause symptoms.
Use wrist splints to keep the wrist in a neutral position.
Take anti-inflammatory medicines to reduce pain and swelling.
Ergonomic changes, like padded gloves or changing hand positions, can help.
Surgery may be needed to remove cysts or relieve pressure if symptoms persist.
What is the prognosis?
Many people improve with rest and conservative treatment.
Early treatment can prevent permanent nerve damage.
Surgery often helps if conservative measures don’t work.
Recovery can take weeks to months depending on severity.
Without treatment, symptoms may worsen and lead to lasting weakness or numbness.
Vasculitis of CNS
What is it?
Vasculitis of the CNS is inflammation of blood vessels in the brain and spinal cord.
It can cause problems with how the brain works, such as headaches or weakness.
This condition is rare and can affect people of any age.
It is sometimes called "primary CNS vasculitis" if it only affects the brain.
Symptoms can be different for each person and may come on slowly or suddenly.
What causes it?
The exact cause is often unknown.
Sometimes, the immune system attacks the blood vessels by mistake.
Infections or other diseases can trigger this inflammation.
Some medicines may rarely cause it.
It is not usually inherited or passed down in families.
How is it diagnosed?
Doctors ask about symptoms and do a physical and neurological exam.
Brain scans like MRI are used to look for signs of inflammation or stroke.
Spinal fluid may be tested with a lumbar puncture.
Sometimes, a small piece of brain tissue (biopsy) is needed for confirmation.
Blood tests are done to rule out other causes.
What is the treatment?
Treatment usually starts with strong medicines to reduce inflammation, like steroids.
Other medications may be added to help control the immune system.
Treatment is tailored to each person’s symptoms and severity.
Regular check-ups and follow-up scans help monitor progress.
Early treatment is important to prevent long-term problems.
What is the prognosis?
Many people improve with early and proper treatment.
Some may have lasting symptoms or need long-term medication.
Relapses can happen, so ongoing care is important.
The outcome depends on how quickly treatment is started and how severe the disease is.
With good care, many people can return to normal activities.
Vascular Dementia (VaD)
What is it?
Vascular dementia is a type of memory and thinking problem caused by reduced blood flow to the brain.
It is the second most common form of dementia after Alzheimer’s disease.
Symptoms may include trouble with planning, memory, and movement.
The condition often starts after a stroke or a series of small strokes.
Changes can happen suddenly or slowly over time.
What causes it?
Blocked or narrowed blood vessels in the brain reduce oxygen and nutrients to brain cells.
Strokes, mini-strokes (TIAs), or ongoing small vessel disease are common triggers.
High blood pressure, diabetes, and high cholesterol increase the risk.
Smoking and heart disease can also contribute.
Sometimes, both vascular and Alzheimer’s changes are present.
How is it diagnosed?
Doctors ask about memory, thinking, and daily life changes.
A physical and neurological exam is performed.
Brain scans like MRI or CT look for strokes or blood vessel changes.
Blood tests help rule out other causes of dementia.
Special memory and thinking tests may be used.
What is the treatment?
There is no cure, but treatment can slow worsening and improve quality of life.
Managing blood pressure, blood sugar, and cholesterol is very important.
Medicines may help with mood, sleep, or behavior changes.
Physical and occupational therapy can help maintain independence.
Stopping smoking and regular exercise are recommended.
What is the prognosis?
Symptoms may get worse over time, but the speed of change varies.
Early treatment of risk factors can help slow down progression.
Some people may have periods of stability between changes.
Support from family, friends, and healthcare teams is important.
Planning ahead for care and safety is helpful as the disease progresses.
Vasculitic Neuropathy
What is it?
Vasculitic neuropathy is nerve damage caused by inflammation of blood vessels supplying the nerves.
It can cause pain, numbness, tingling, and weakness in the arms or legs.
The symptoms may start suddenly or develop over weeks or months.
It can affect one nerve, several nerves, or many nerves at once.
Both men and women can get this condition, usually in middle age or older.
What causes it?
The immune system attacks the blood vessels by mistake, causing inflammation.
Sometimes, it is part of a larger illness like lupus or rheumatoid arthritis.
Infections or certain medications may rarely trigger it.
Often, the exact reason is not known.
It is not caused by injury or overuse of nerves.
How is it diagnosed?
Doctors ask about symptoms and do a detailed physical and neurological exam.
Blood tests check for signs of inflammation or underlying diseases.
Nerve tests (EMG and nerve conduction studies) help find which nerves are affected.
Sometimes, a small piece of nerve is taken (biopsy) to look for inflammation.
Other causes of nerve problems are ruled out first.
What is the treatment?
Medicines that reduce the immune system’s attack, like steroids, are usually started.
Other immune-suppressing drugs may be added if needed.
Pain medicines can help with nerve pain.
Physical therapy helps maintain strength and function.
Treatment is adjusted based on how severe the symptoms are and how you respond.
What is the prognosis?
Many people improve with early treatment.
Some nerve damage may remain, especially if treatment is delayed.
Ongoing treatment may be needed to prevent relapses.
Most people can regain some or most of their normal activities.
Regular follow-up is important to monitor for new symptoms or side effects.
Vestibular Dysfunction
What is it?
Vestibular dysfunction is a problem with the balance system in the inner ear.
It can cause dizziness, spinning sensations (vertigo), and unsteadiness.
People may feel like the room is moving or have trouble walking straight.
Symptoms may happen in short episodes or last longer.
It can affect people of any age but is more common as we get older.
What causes it?
Small crystals in the inner ear may move out of place (BPPV).
Inner ear infections or inflammation can affect balance (vestibular neuritis).
Meniere’s disease causes extra fluid in the ear, leading to vertigo and hearing changes.
Head injuries or certain medications can sometimes cause vestibular problems.
Some causes are related to the brain, such as strokes, but most are from the ear.
How is it diagnosed?
Doctors ask about your symptoms and when they occur.
A physical exam and simple balance tests are done in the clinic.
Special maneuvers may be used to trigger symptoms and help with diagnosis.
Hearing tests may be done if you have ringing or hearing loss.
Sometimes, an MRI is needed to rule out problems in the brain.
What is the treatment?
Simple head movements (like the Epley maneuver) can treat some causes.
Medicines can help reduce dizziness and nausea during attacks.
Balance exercises (vestibular rehabilitation) help the brain adjust.
Diet changes and medications may help with Meniere’s disease.
Most people improve with treatment, but some may need ongoing therapy.
What is the prognosis?
Many people recover fully or have much fewer symptoms with treatment.
Some may have mild balance problems that last longer.
Repeated episodes can happen, especially with certain types like BPPV.
Falls are a risk, so safety at home is important.
Ongoing therapy and follow-up can help manage long-term symptoms.
Wallenberg Syndrome
What is it?
Wallenberg Syndrome is a type of stroke that affects a part of the brainstem called the lateral medulla.
It can cause problems with balance, swallowing, and sensation.
People may experience dizziness, hoarseness, and trouble walking.
It is sometimes called lateral medullary syndrome.
The symptoms can be sudden and may affect one side of the face or body more than the other.
What causes it?
Wallenberg Syndrome is usually caused by a blockage in an artery that supplies blood to the brainstem.
The most common arteries involved are the vertebral artery or the posterior inferior cerebellar artery.
Risk factors include high blood pressure, smoking, and hardening of the arteries.
Less commonly, a tear in the artery (dissection) can cause the syndrome.
Reduced blood flow leads to damage in the affected area of the brain.
How is it diagnosed?
Doctors diagnose Wallenberg Syndrome by asking about symptoms and doing a neurological exam.
Imaging tests like MRI scans help show which part of the brain is affected.
Special scans of the blood vessels may be done to find a blockage or tear.
The pattern of symptoms, such as changes in sensation on one side of the face and the opposite side of the body, is a key clue.
Early diagnosis is important for starting treatment and preventing complications.
What is the treatment?
Treatment focuses on improving blood flow and preventing further strokes.
Medications may include blood thinners or antiplatelet drugs.
Rehabilitation with physical, occupational, and speech therapy helps with recovery.
Supportive care is given for swallowing problems and to prevent choking.
Managing risk factors like high blood pressure and quitting smoking is important for long-term health.
What is the prognosis?
Recovery depends on the size and location of the stroke and how quickly treatment starts.
Some people improve significantly with therapy, but others may have lasting difficulties.
Problems with balance, swallowing, or speech may take time to get better.
Early rehabilitation increases the chances of regaining independence.
Ongoing medical care helps prevent future strokes and manage symptoms.
Wernicke’s Encephalopathy
What is it?
Wernicke’s Encephalopathy is a brain disorder caused by a lack of vitamin B1 (thiamine).
It often affects people with poor nutrition or long-term alcohol use.
The condition can lead to confusion, balance problems, and eye movement changes.
It is a medical emergency that needs quick treatment.
Without treatment, it can cause lasting brain damage.
What causes it?
The main cause is not getting enough thiamine, a vitamin needed for brain health.
Heavy drinking, poor diet, or medical problems that affect nutrition can lead to thiamine deficiency.
Some illnesses or surgeries that make it hard to absorb nutrients can also cause it.
The brain cannot work properly without thiamine.
Early treatment can prevent serious complications.
How is it diagnosed?
Doctors look for symptoms like confusion, trouble walking, and unusual eye movements.
A history of poor nutrition or heavy alcohol use can be a clue.
There is no single test, but brain scans may help rule out other causes.
Blood tests for thiamine levels are not always reliable.
Quick improvement after giving thiamine supports the diagnosis.
What is the treatment?
The main treatment is giving thiamine, usually by injection or IV, as soon as possible.
Thiamine should be given before any sugar or glucose.
Supportive care includes treating other health problems and making sure the person eats well.
Ongoing thiamine supplements may be needed after leaving the hospital.
Early treatment can reverse symptoms and prevent permanent damage.
What is the prognosis?
If treated early, many people recover well from Wernicke’s Encephalopathy.
Some symptoms, like balance or memory problems, may take time to improve.
Delayed treatment can lead to lasting brain damage or a condition called Korsakoff syndrome.
Ongoing alcohol use or poor nutrition increases the risk of recurrence.
Regular follow-up and good nutrition help prevent future problems.
West Nile Encephalitis
What is it?
West Nile Encephalitis is a brain infection caused by the West Nile virus.
The virus is usually spread to humans by mosquito bites.
Most people infected with West Nile virus have no symptoms or only mild illness.
In rare cases, the virus can cause serious brain inflammation.
The condition is more common in late summer and early fall.
What causes it?
West Nile virus is carried by mosquitoes that have bitten infected birds.
Humans get the virus through mosquito bites.
The virus can sometimes spread to the brain and cause swelling.
Older adults and people with weak immune systems are at greater risk for severe illness.
Being outdoors where mosquitoes are common increases the risk.
How is it diagnosed?
Doctors ask about symptoms and recent mosquito exposure.
Blood tests or spinal fluid tests can detect signs of West Nile virus infection.
Brain scans like MRI may be done to look for inflammation.
Other causes of brain infection are ruled out with various tests.
Early diagnosis helps guide supportive care.
What is the treatment?
There is no specific cure for West Nile Encephalitis.
Treatment focuses on relieving symptoms and supporting the patient.
Hospital care may include fluids, medications for fever, and help with breathing if needed.
Some people may need physical therapy to recover strength.
Preventing mosquito bites is the best way to avoid infection.
What is the prognosis?
Most people recover fully from mild West Nile infection.
Severe brain infection can lead to long-term problems with movement, memory, or weakness.
Recovery may take weeks or months, especially in older adults.
Some people may have lasting fatigue or difficulty with daily activities.
Early supportive care can improve outcomes and reduce complications.
Wilson’s Disease
What is it?
Wilson’s Disease is a rare condition where the body cannot get rid of extra copper.
Copper builds up in organs like the liver, brain, and eyes.
It can cause problems with movement, mood, and liver function.
The disease often starts in children or young adults.
Early diagnosis and treatment can prevent serious complications.
What causes it?
Wilson’s Disease is caused by a change in a gene passed down from both parents.
The gene problem makes it hard for the liver to remove extra copper.
Copper then leaks into the bloodstream and collects in other organs.
The buildup of copper damages the liver and nervous system.
Family members may also be at risk and should be tested.
How is it diagnosed?
Doctors ask about symptoms like tremors, mood changes, or liver problems.
Eye exams can show a ring of copper (Kayser-Fleischer ring) around the cornea.
Blood and urine tests measure copper and a protein called ceruloplasmin.
Sometimes a liver biopsy is needed to check for copper buildup.
Genetic testing can confirm the diagnosis, especially in families.
What is the treatment?
Medicines called chelators help remove extra copper from the body.
Zinc supplements can help block copper absorption from food.
A low-copper diet is recommended, avoiding foods like shellfish and liver.
Some people with severe liver problems may need a liver transplant.
Lifelong treatment is needed to keep copper levels safe.
What is the prognosis?
With early and ongoing treatment, most people live normal lives.
Symptoms usually improve with proper therapy and diet.
Delayed treatment can lead to permanent liver or brain damage.
Regular check-ups are important to monitor copper levels.
Family screening helps find and treat others who may have the disease.
X-linked Adrenoleukodystrophy
What is it?
X-linked adrenoleukodystrophy (X-ALD) is a rare genetic disorder that affects the brain and adrenal glands.
It mostly affects boys and men because it is linked to the X chromosome.
The disease causes damage to the protective covering of nerve cells, leading to problems with movement, behavior, and learning.
It can also cause the adrenal glands to stop working properly, affecting hormone production.
Symptoms and severity can vary widely from person to person.
What causes it?
X-ALD is caused by changes (mutations) in a gene called ABCD1.
This gene helps the body break down very long fatty acids found in foods and cells.
When the gene does not work properly, these fatty acids build up in the brain and adrenal glands.
The buildup damages nerve cells and adrenal glands over time.
The condition is inherited from the mother, who may carry the gene without showing symptoms.
How is it diagnosed?
Doctors suspect X-ALD when boys show signs like behavior changes, learning difficulties, or adrenal problems.
Blood tests measure levels of very long-chain fatty acids, which are usually high in X-ALD.
Brain scans (MRI) can show damage to the white matter of the brain.
Genetic testing confirms the diagnosis by identifying mutations in the ABCD1 gene.
Family members may also be tested to find carriers or affected individuals early.
What is the treatment?
There is no cure, but treatments can slow disease progression and manage symptoms.
Stem cell transplant may help if done early in the brain disease stage.
Hormone replacement therapy is needed if the adrenal glands are not working.
Special diets and medicines may help reduce fatty acid levels, but their effects vary.
Supportive care includes physical therapy, managing seizures, and helping with learning and behavior.
What is the prognosis?
The outlook depends on the type and severity of the disease.
Early diagnosis and treatment can improve quality of life and slow progression.
Some forms progress rapidly, especially in young boys, while others progress slowly.
Females who carry the gene usually have milder symptoms or none at all.
Ongoing research aims to find better treatments and improve outcomes for patients.












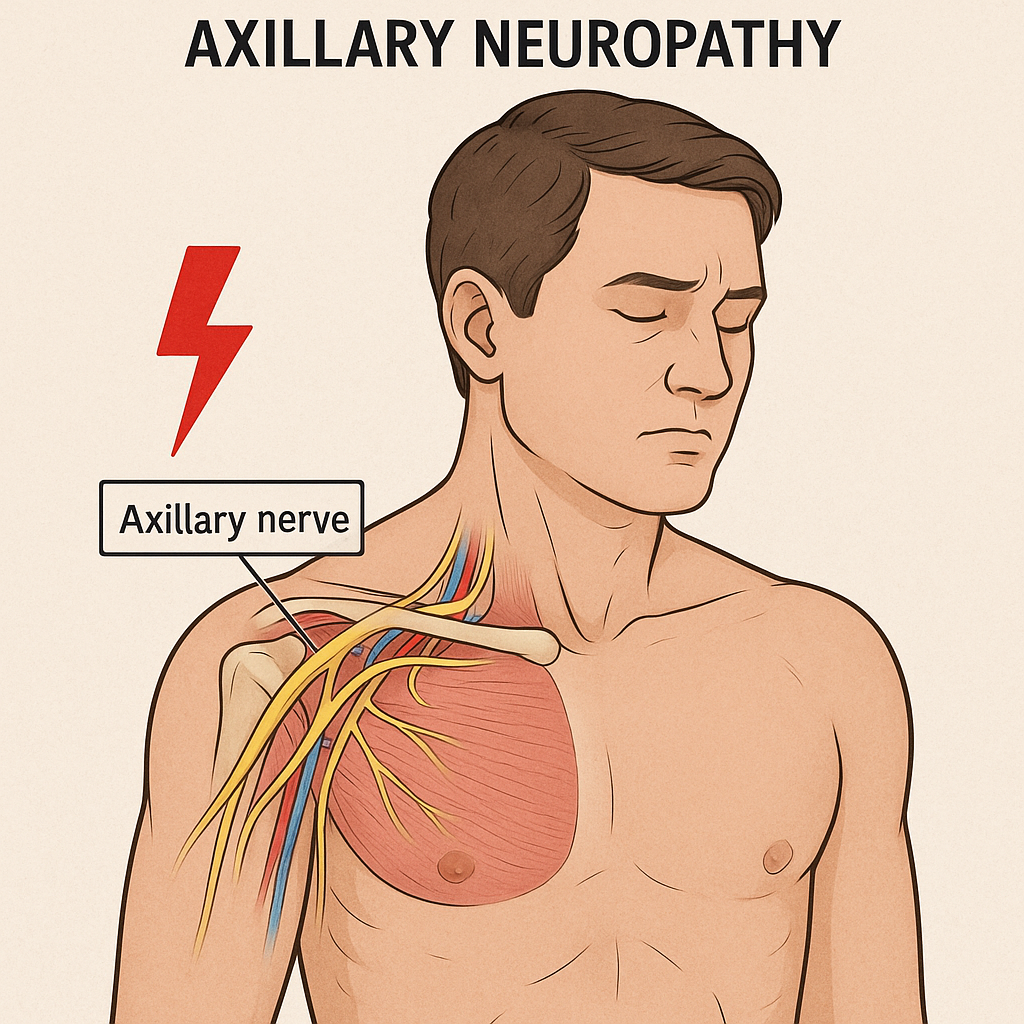
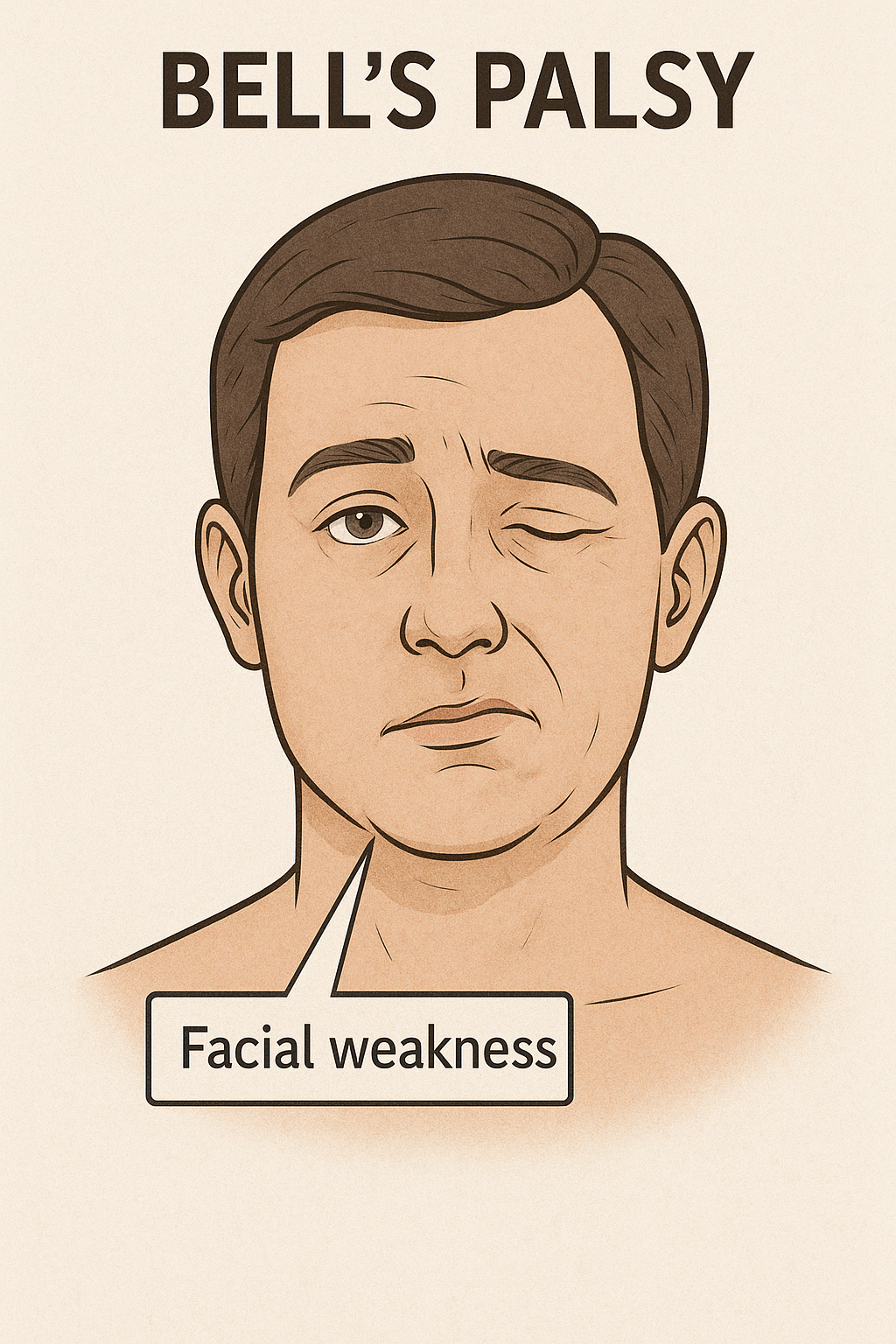
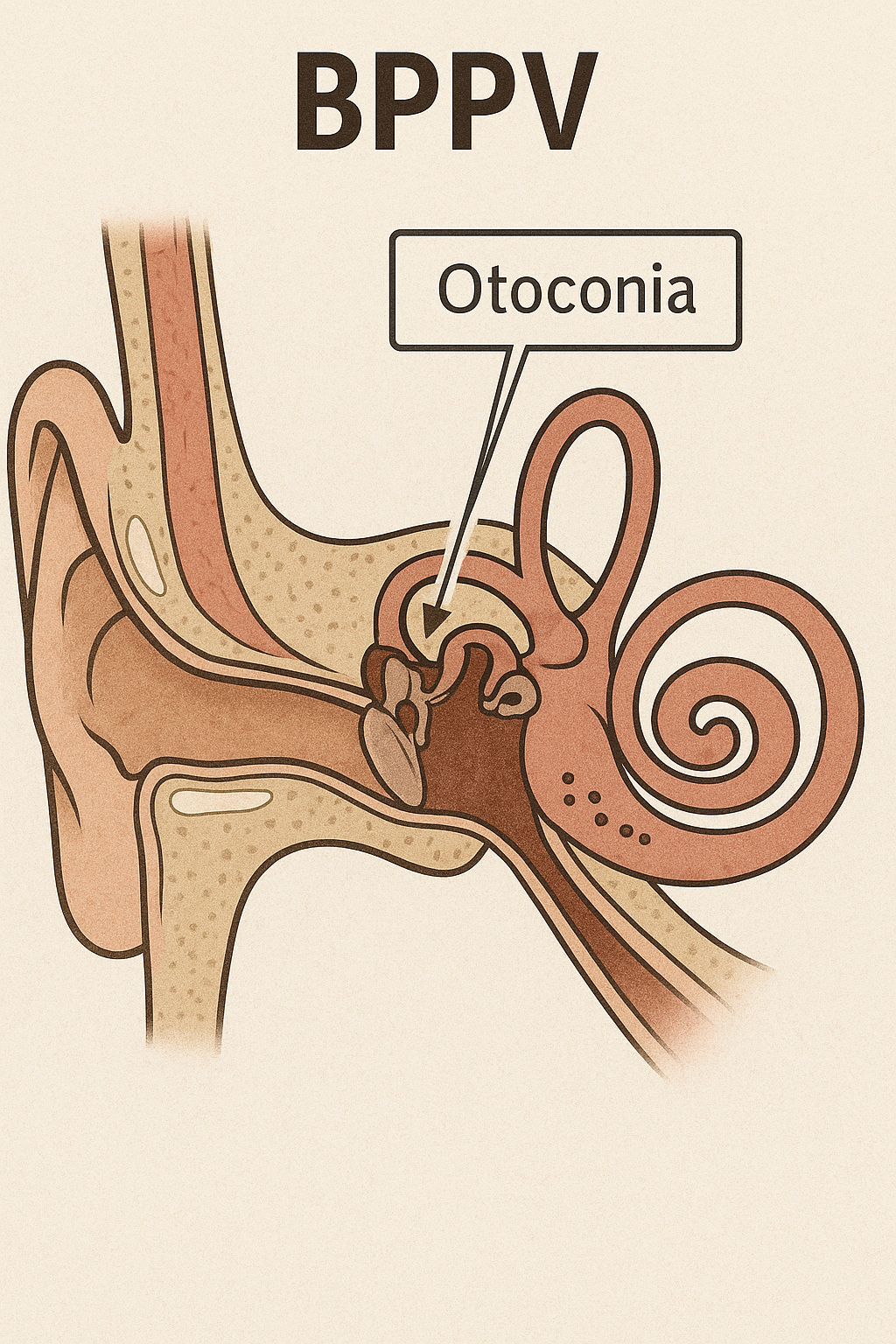
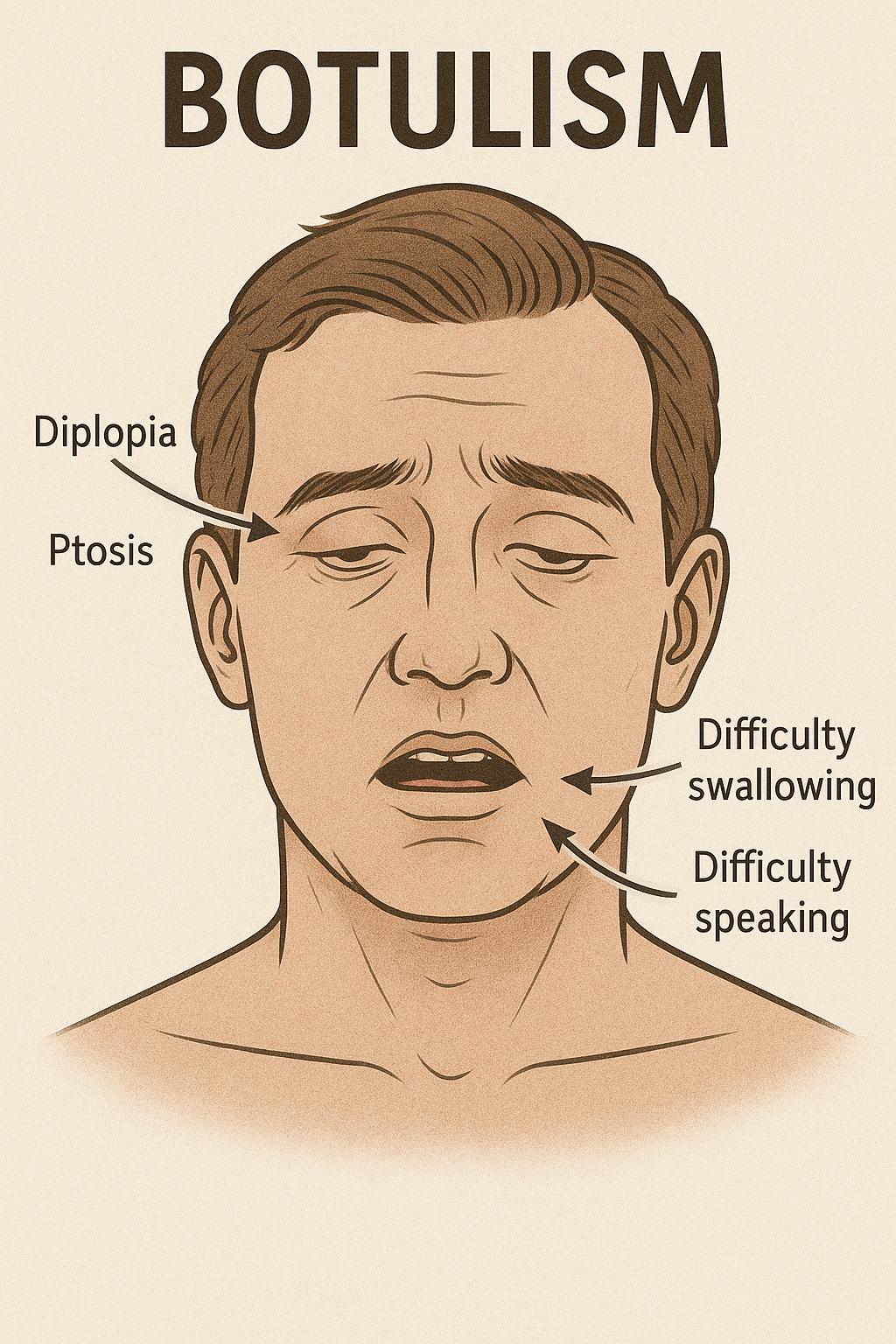
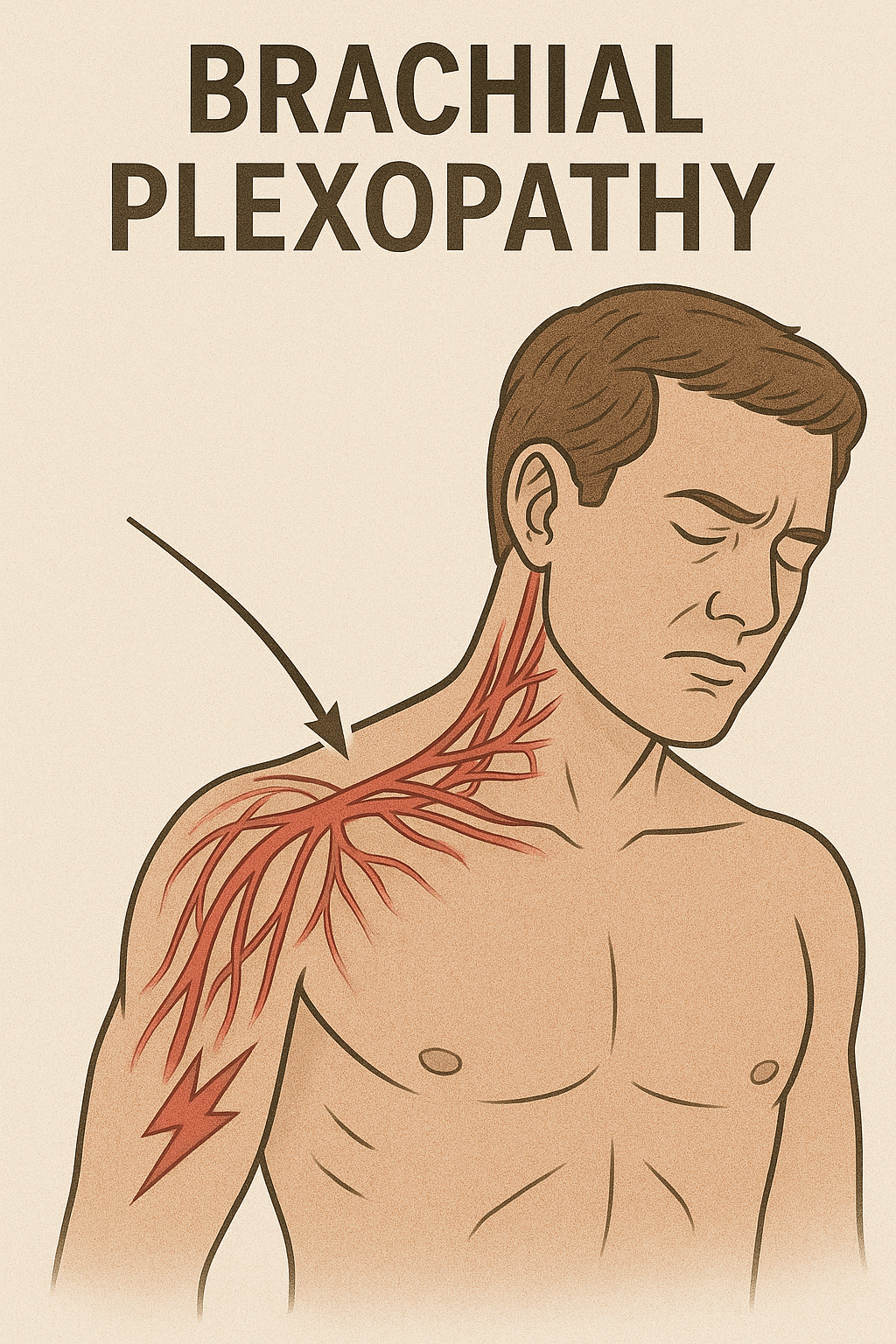
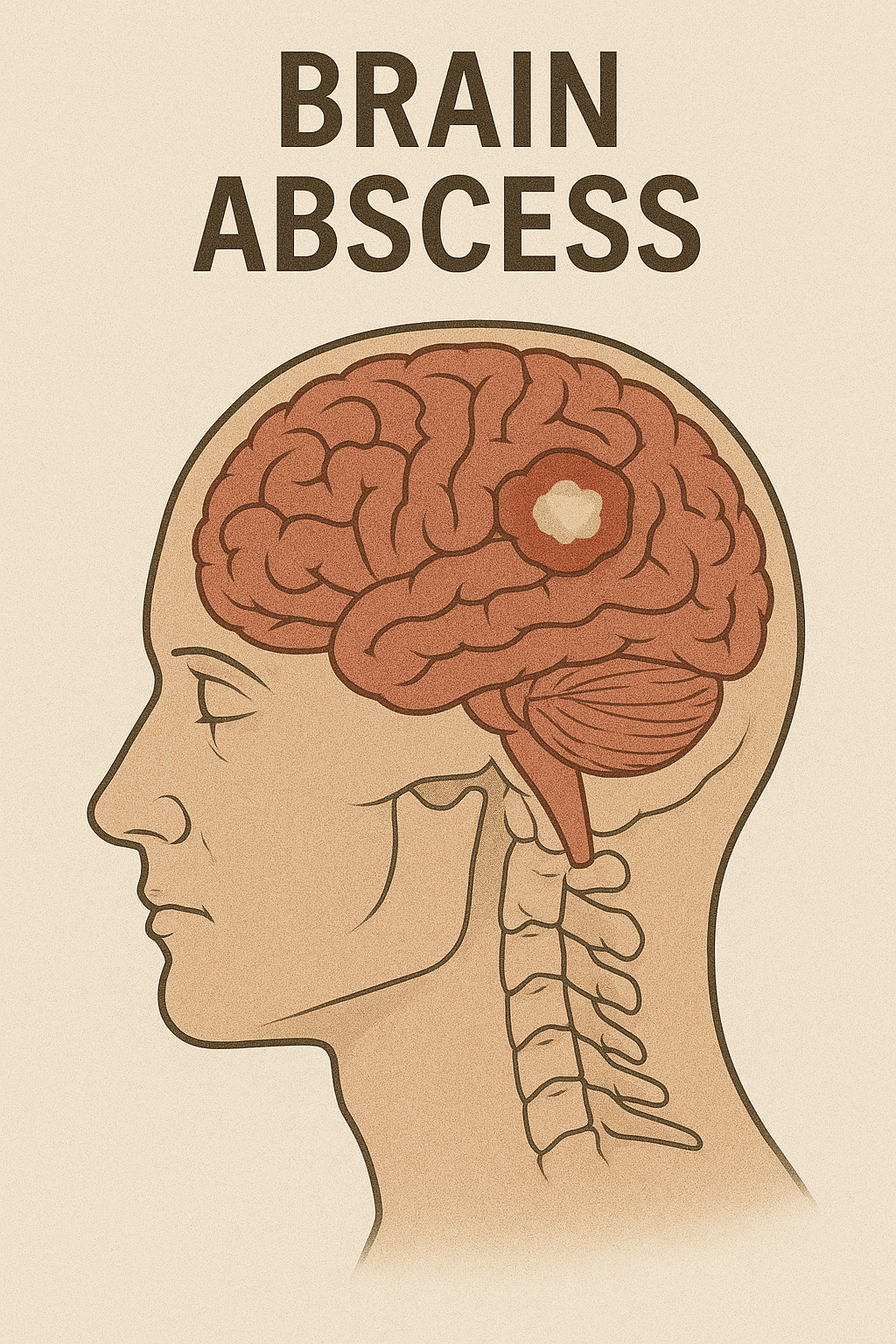

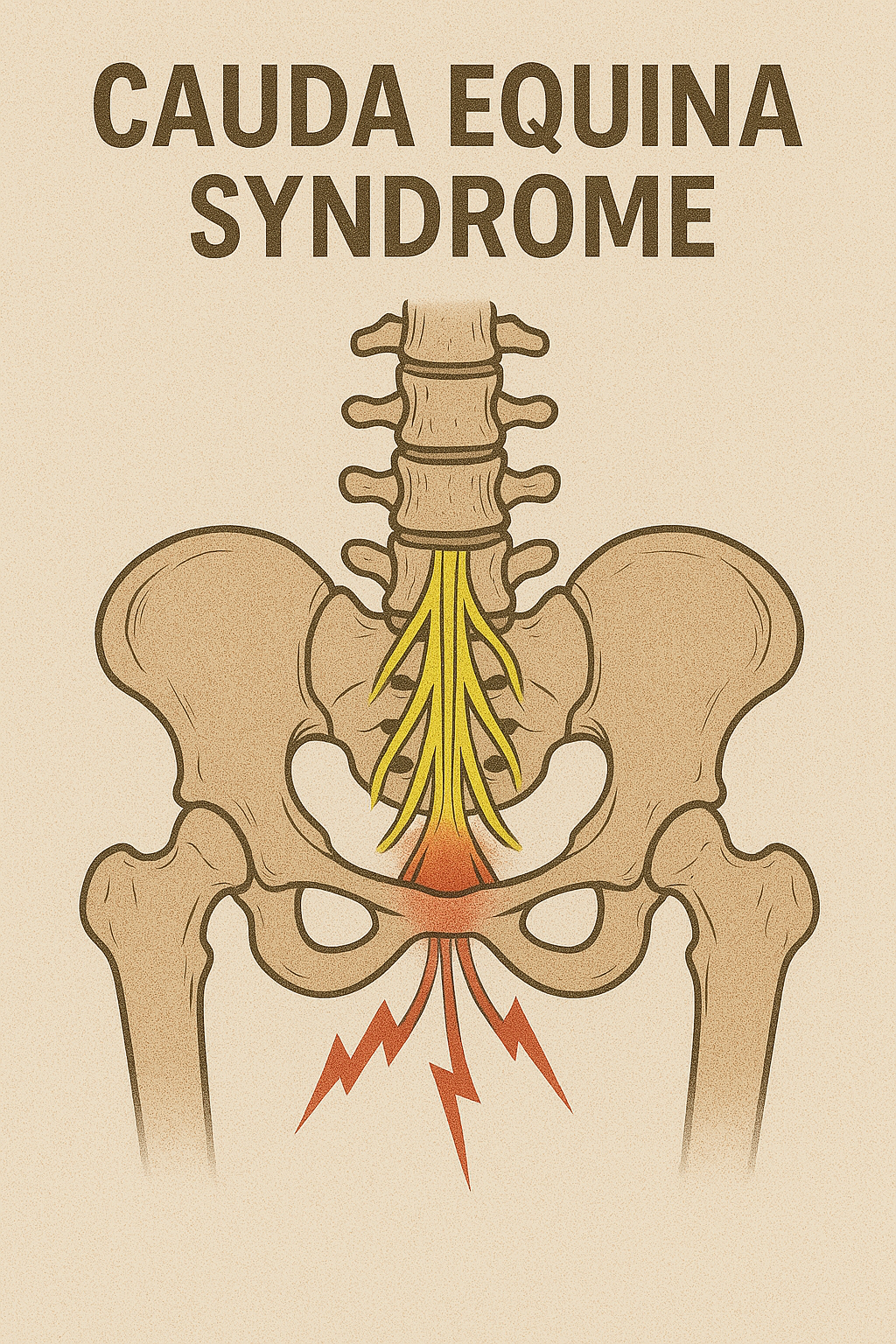

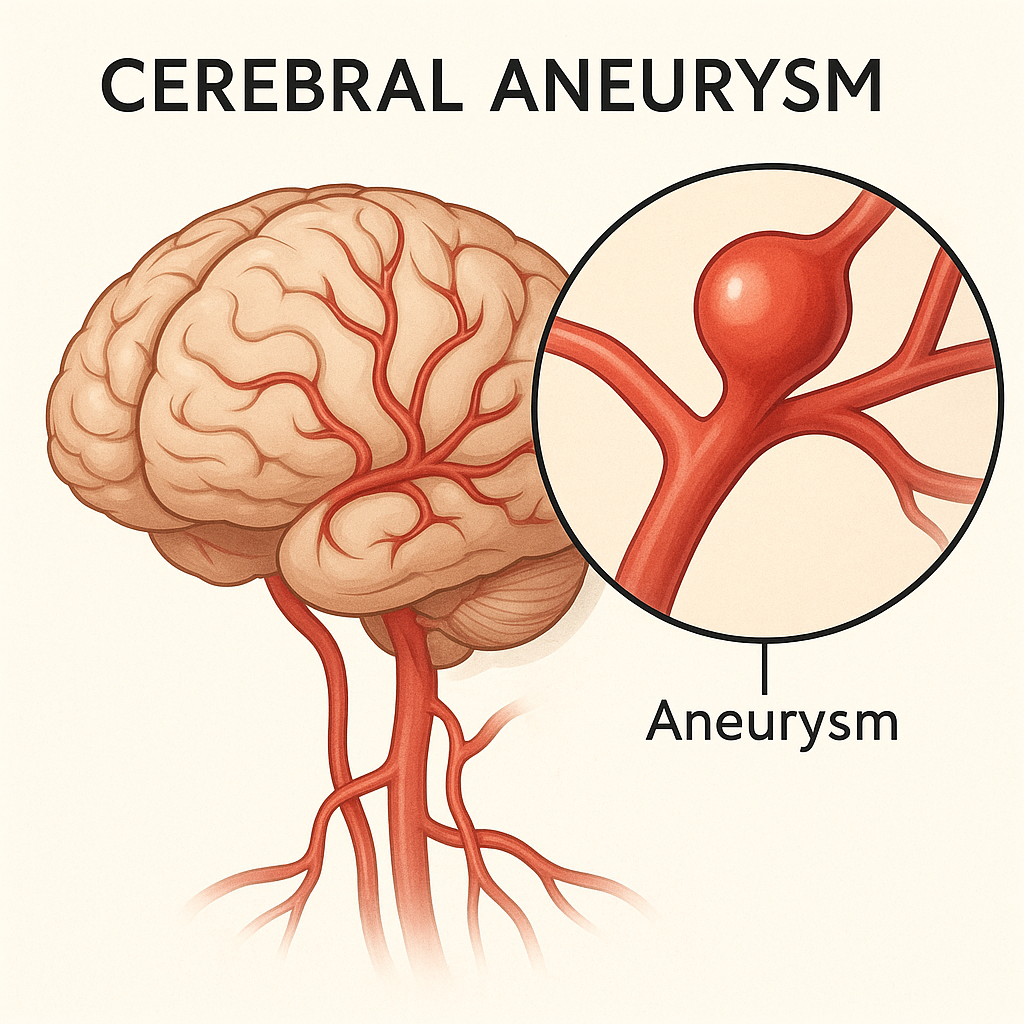

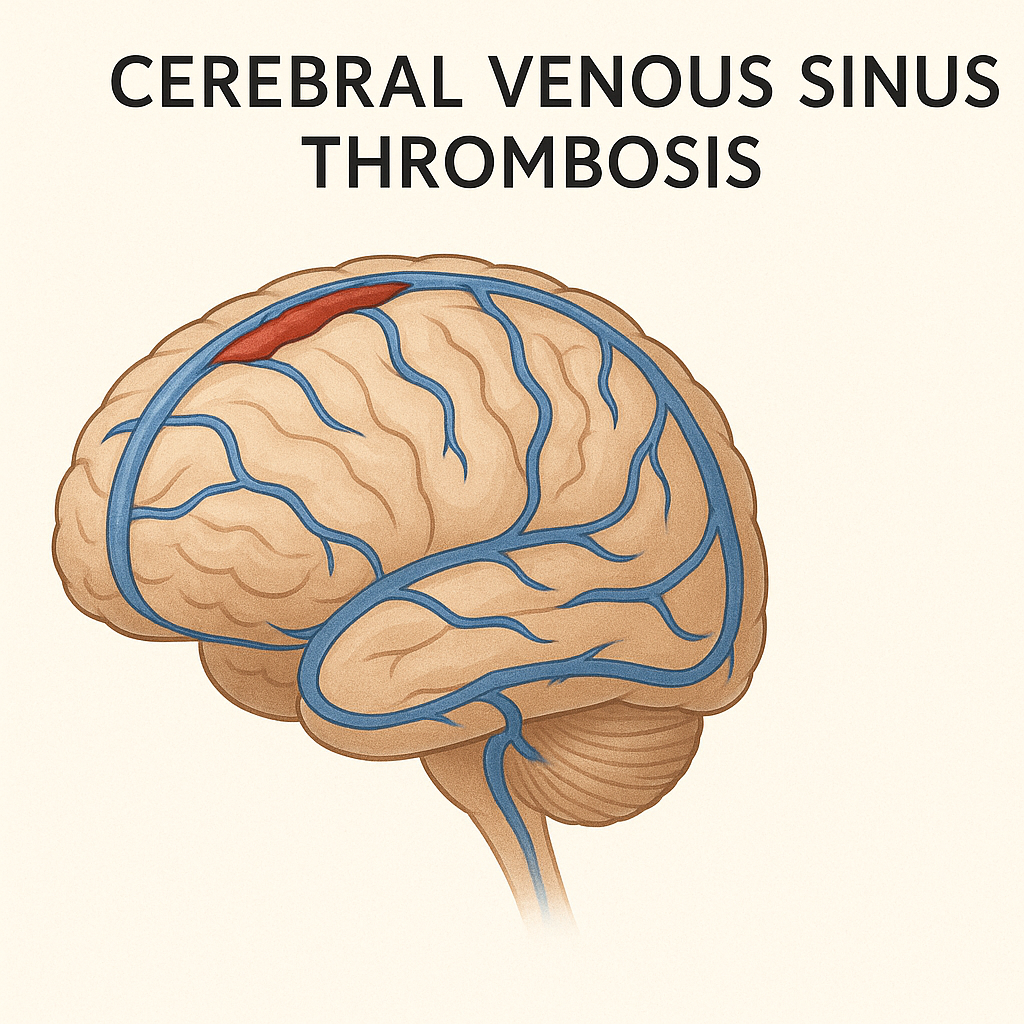
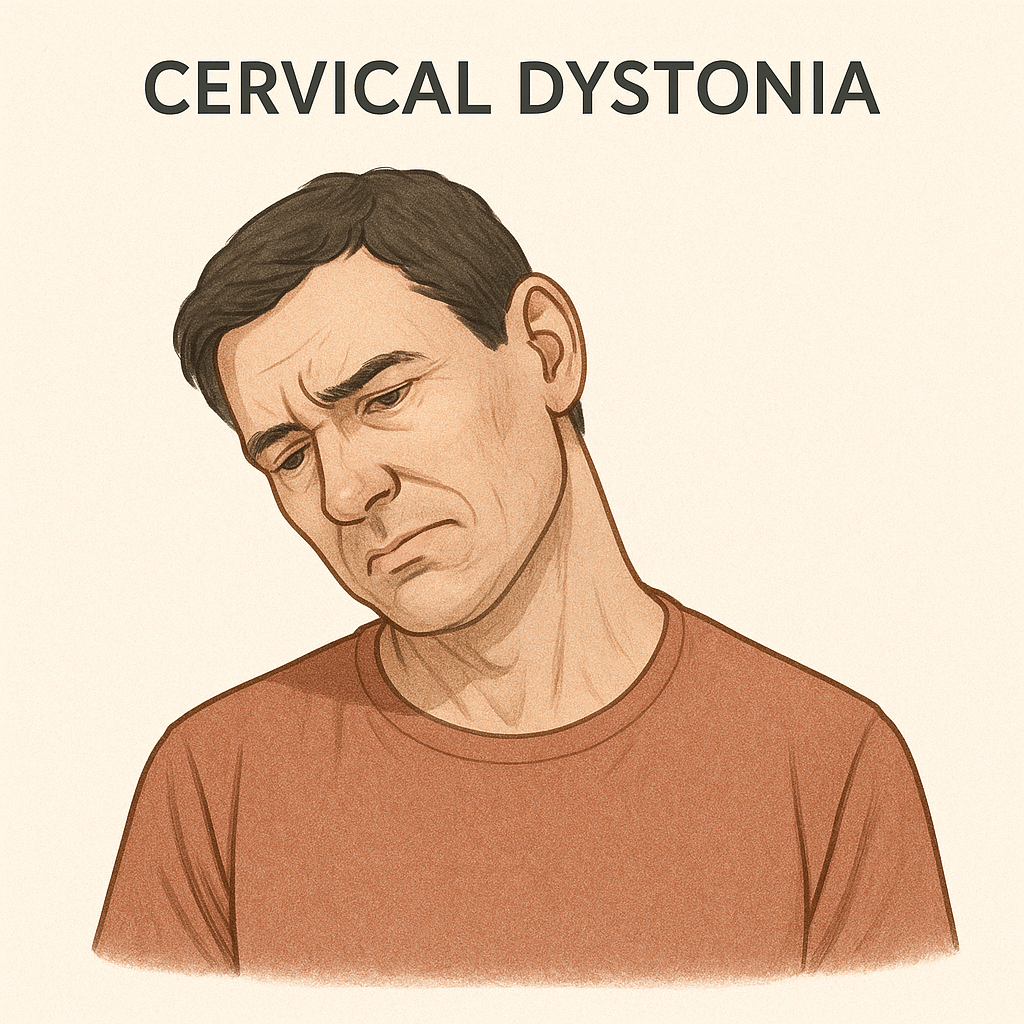
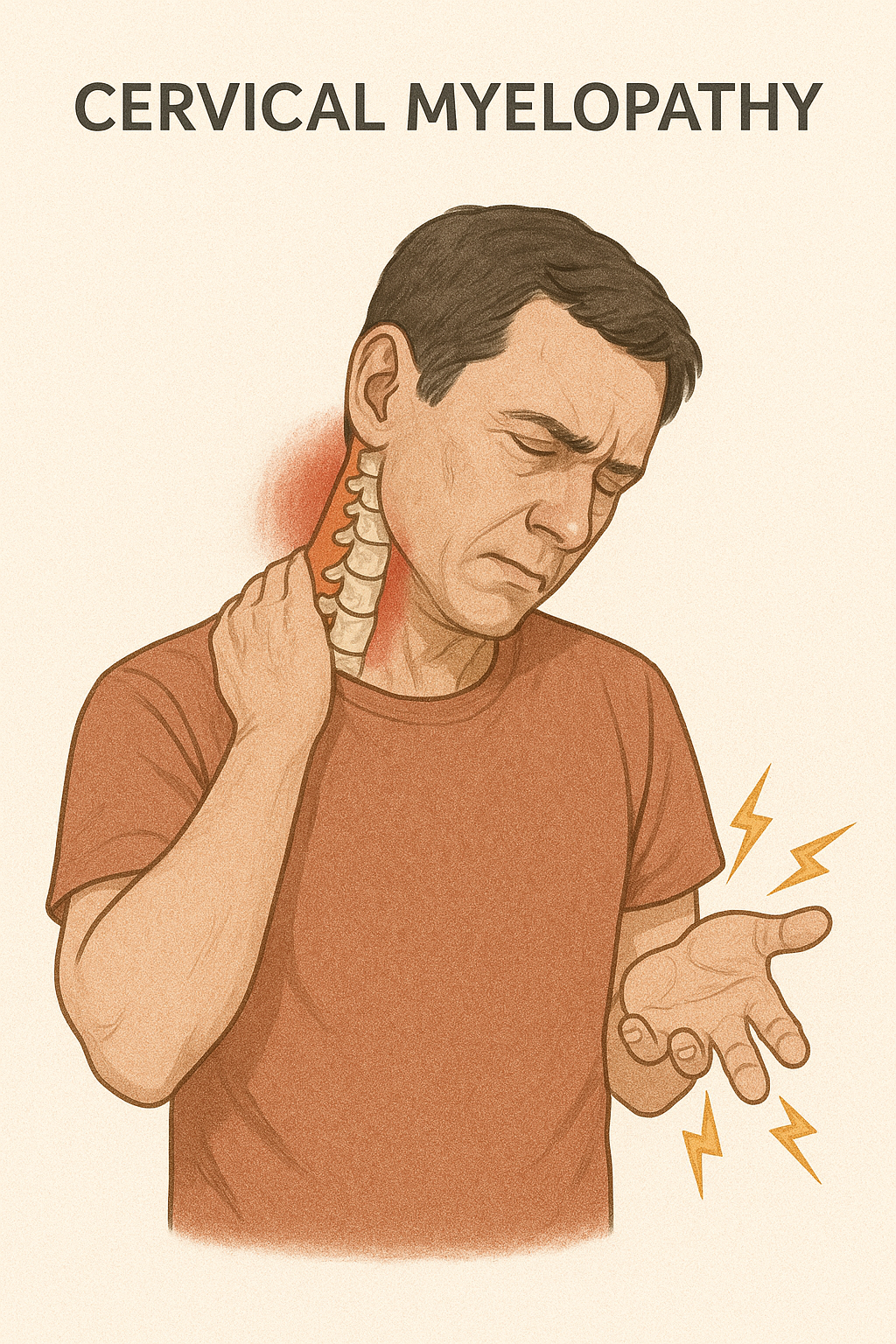
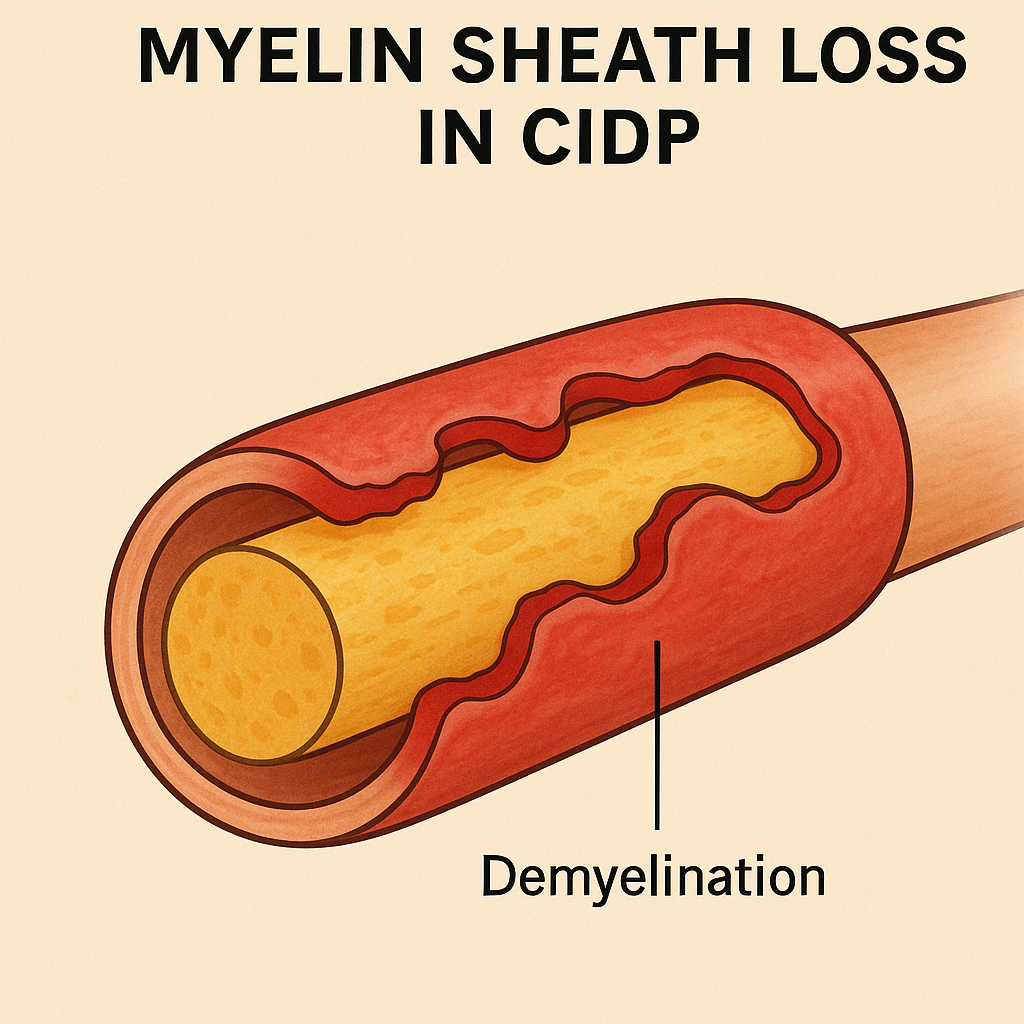






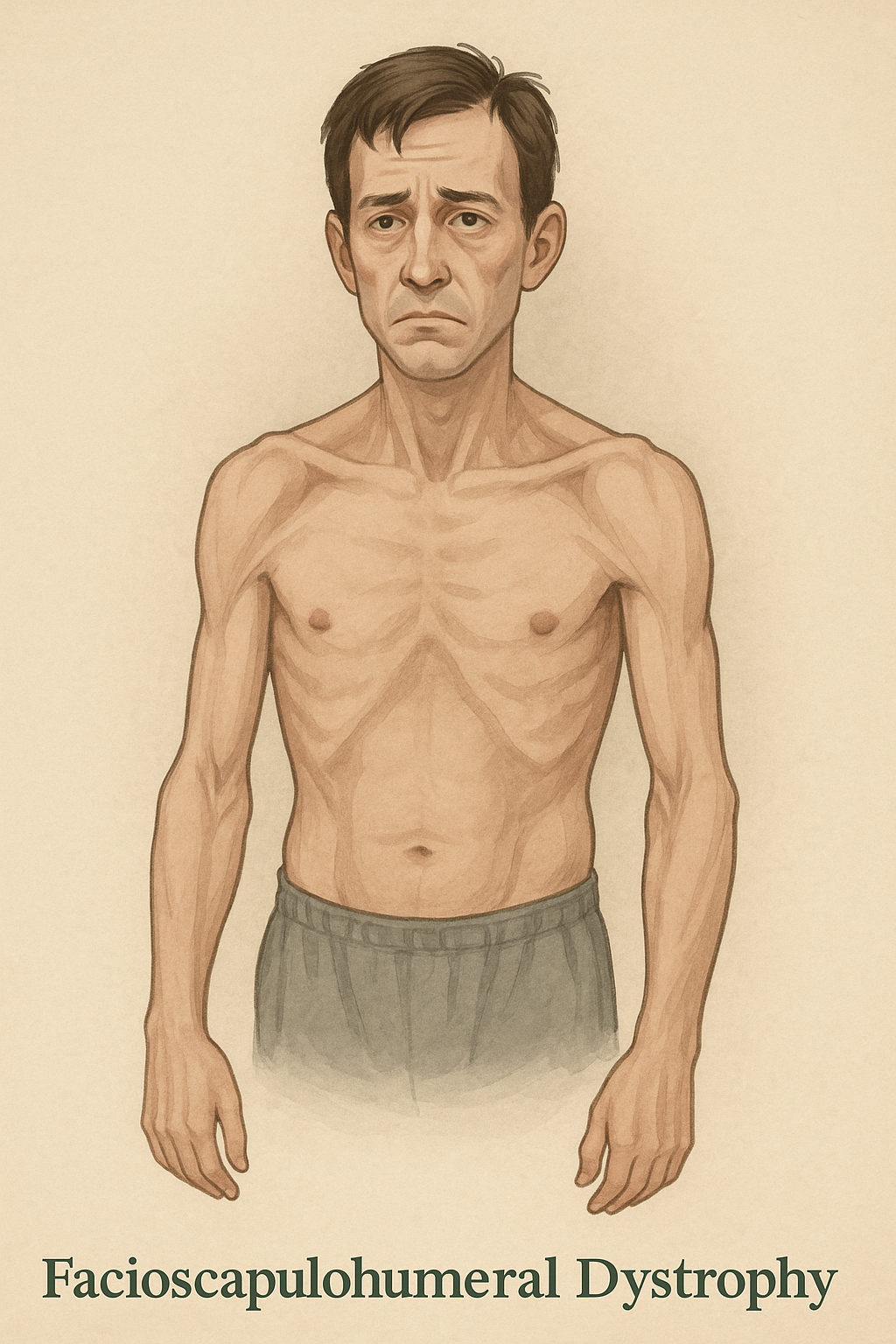



















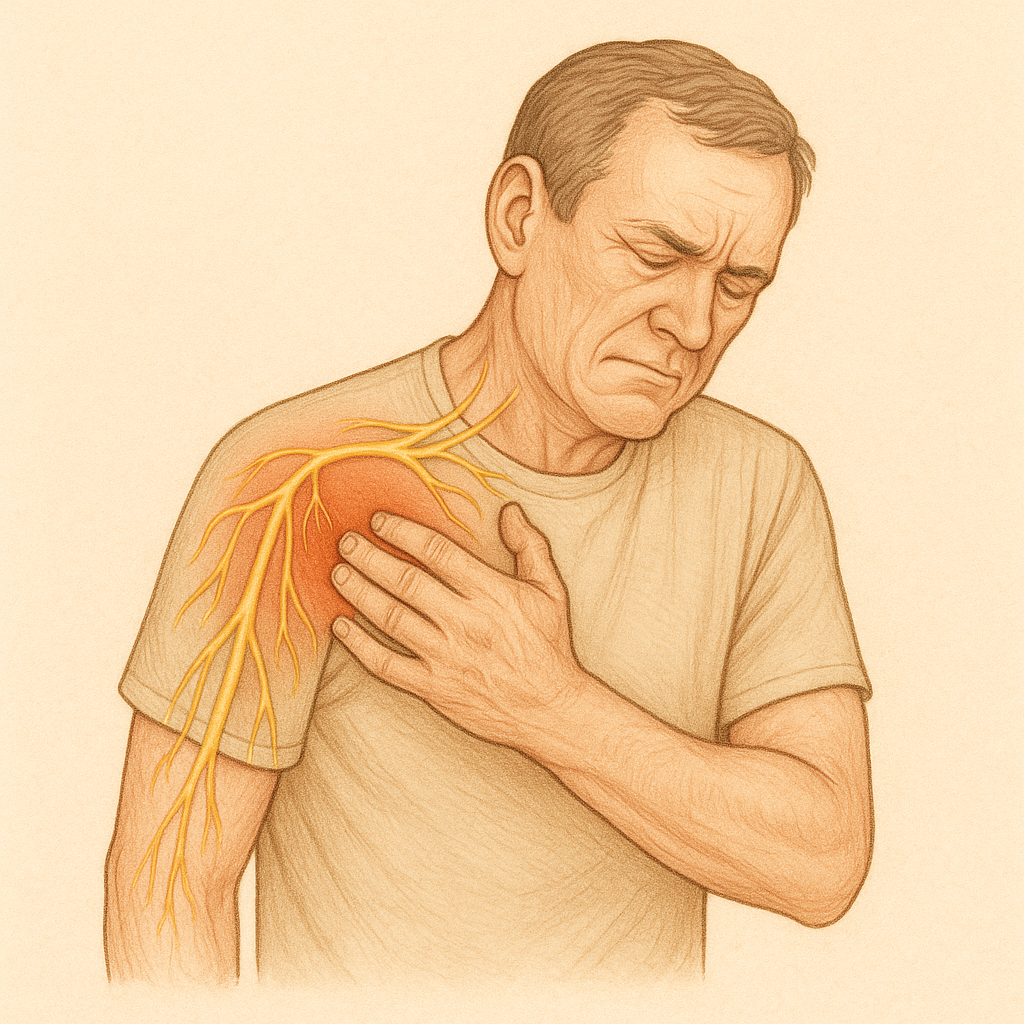
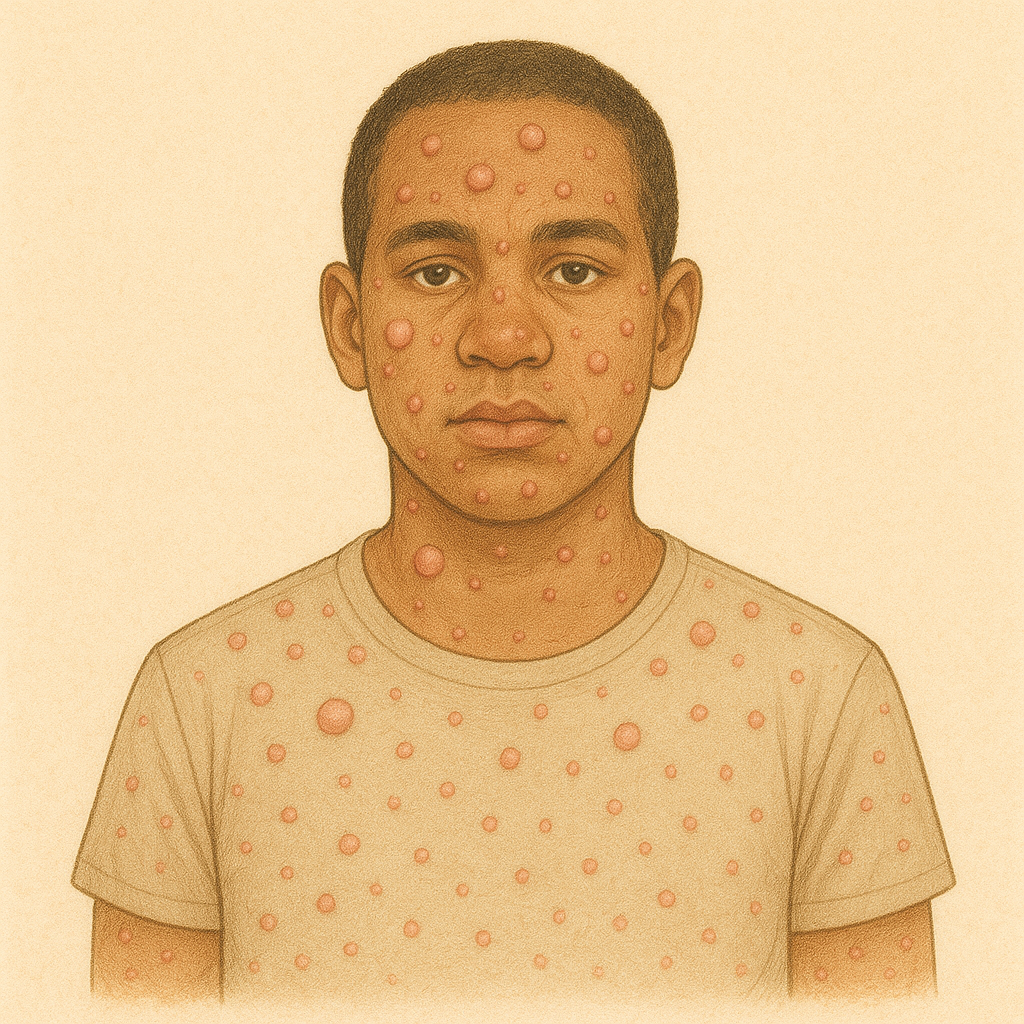
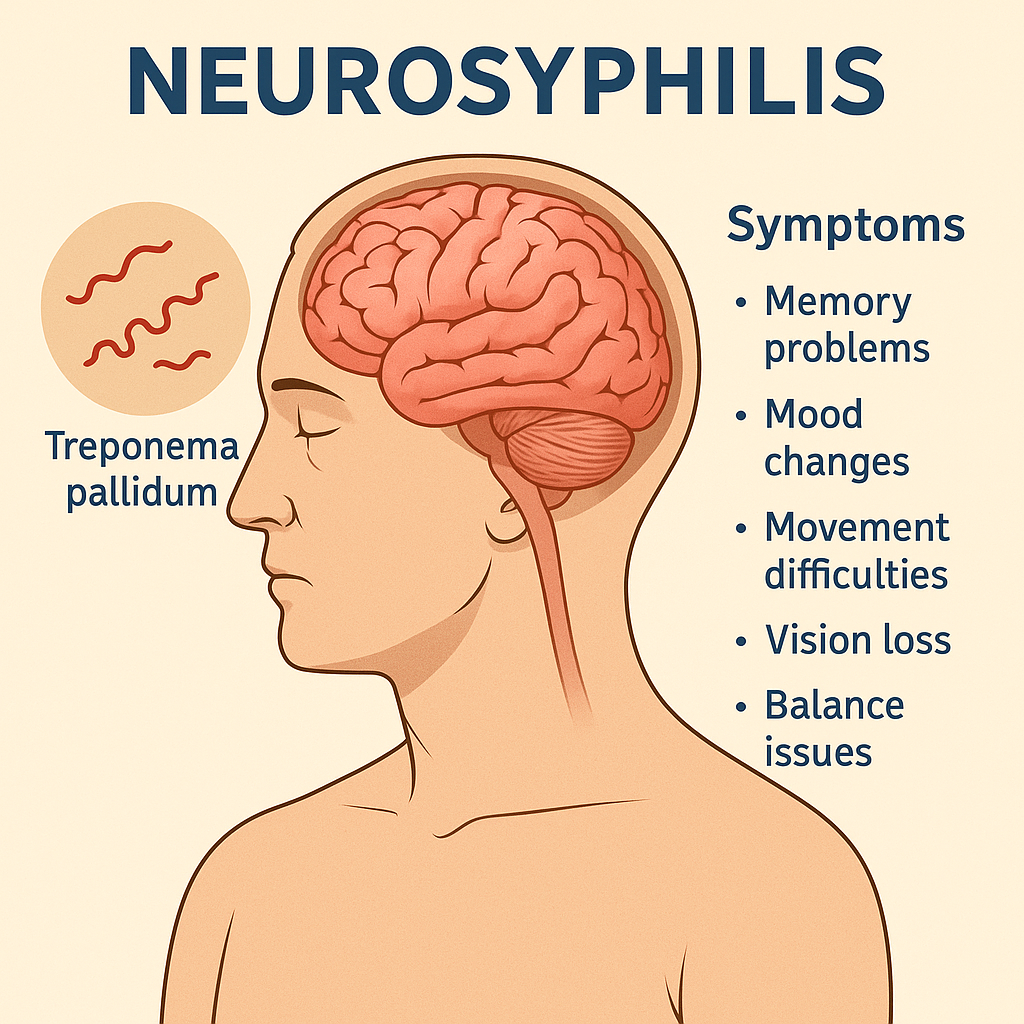




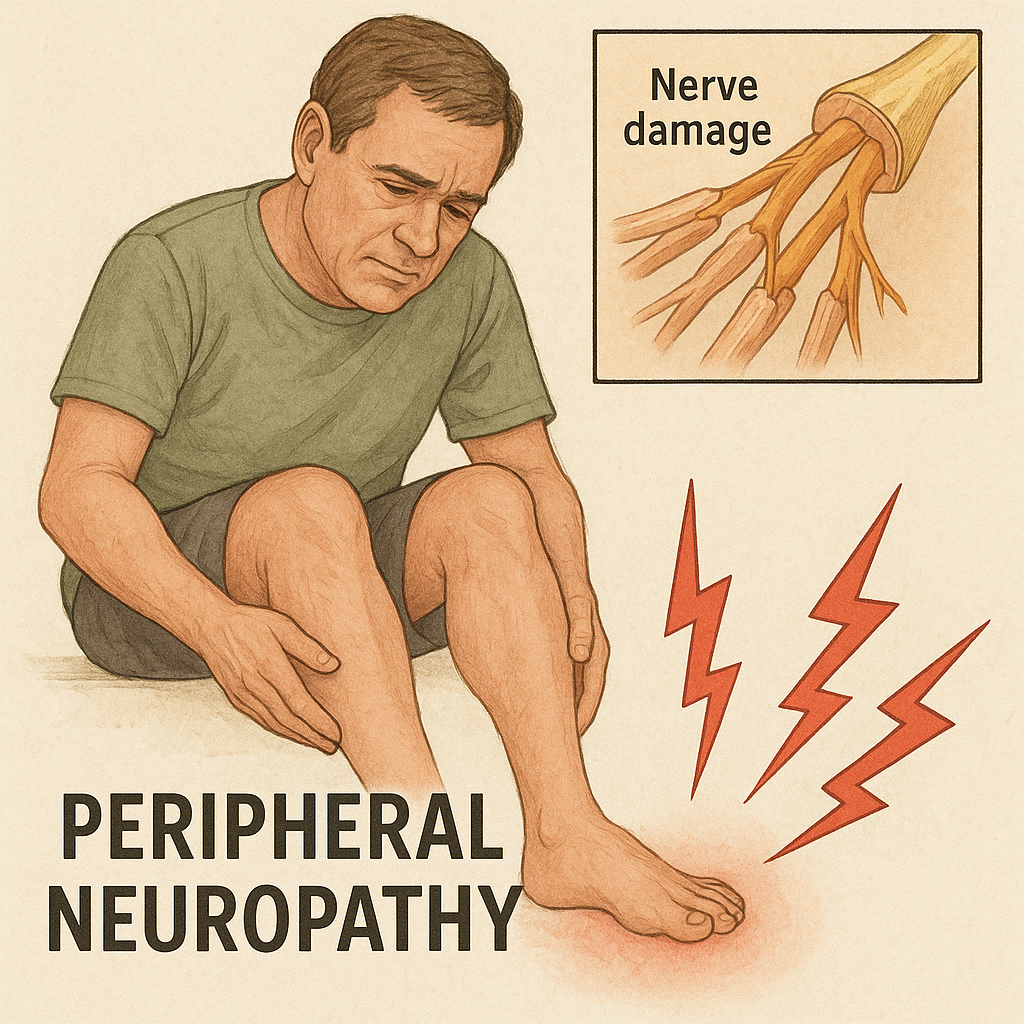













 ## What is it?
## What is it?